There’s a (possibly rare (1 in ~100000), but possibly relatively common (4.4 in 100, according to a 2006 Edinburgh study, (full pdf available here))) condition called synæsthesia (sometimes also spelled synesthesia) in which the subjects’ senses are “crossed”; common examples include sounds perceived as colours (so Rhapsody in Blue really is in blue), or numbers perceived as colours (“grapheme-colour synæsthesia”) or as 3-dimensional objects (“number form synæsthesia”.) There may be a genetic component, since it is known that the phenomenon has a higher incidence among first-degree relatives, but there is no consensus on the cause of the condition.
The 2003 BBC Radio Reith Lectures were given by neurologist Vilayanur S. Ramachandran; he has made a particular study of synæsthesia, and devoted the fourth of his lectures (Purple Numbers and Sharp Cheese) to the condition. Studying the brains of people with the condition in fMRIs, he found that adjacent regions of the brain, which usually interpret different sense input, overlap in synæsthetes, so when one sense is stimulated, the overlapping part also reacts. He also found — rather interestingly, I think — that people with synæsthesia involving numbers only experience the phenomenon when the numbers are written in their native language (so for example, if the subject perceives colours or sounds on seeing Arabic numerals (0, 1, 2, 3, 4, 5, etc), the same numbers written in, say, Roman numerals, will still be perceived as numbers, but without the other association.) More research is being conducted, but not all researchers accept the “cross-wiring” theory (although it does —at least in part — make sense to me; an issue I have is that the two “crossed” senses should(? possibly?) be mutually crossed, so if somone sees a particular colour on hearing a particular sound or piece of music they should hear the sound/music on seeing the colour. As far as I can discover this doesn’t happen.)
Some research into the brains of convicted pædophile CSOs, conducted in the hope of finding some pronounced differences between them and “normal” brains, might have found some, but it’s disputed. This 2013 episode of ABC Radio National’s All in the Mind, on the subject of the psychology of pædophilia, featured an interview with James Cantor, Associate Professor of Psychiatry at the University of Toronto; he suggested that, in normal, healthy adults, seeing children evokes a parental or “nurturing” instinct, whereas in pædophiles — even those who don’t act on the urges — it evokes a sexual response, and that this response is because the two parts of the brain that respond to these stimuli, normally separate, are “cross-wired”, similar to the overlapping brain regions in synæsthetes referred to above. Other researchers in the same show don’t necessarily agree with Cantor, and offer their own theories.
People who are attracted to the opposite sex think that the way they feel is “natural”; people who are attracted to the same sex also feel that it’s “natural.” It’s no stretch of the imagination to suppose that pædophiles feel the same way about their attraction to children. We know that “conversion therapies,” intended to change homosexuals and bisexuals into heterosexuals, don’t work, and never have (see, for example, this 2001 letter by the then-Surgeon General of the USA,) so it seems reasonable to suppose that attempts to “cure” pædophiles are similarly doomed to failure. Notwithstanding the foregoing, this article from the 29 July 2016 edition of the Psychiatric Times, titled Pedophilia: Interventions That Work, suggests that there are interventions that — while not changing the pædophile’s sexual orientation — can help the individual avoid (re)offending. That article also claims that the primary evidence that the interest of people with pedophilia cannot change is the statement by John Money that paraphilias are vandalized love maps that once created cannot be changed, although the author adds, So far as I know, no one has ever shown that paraphilic interests are immutable. John Money gained notoriety as the advising psychologist in the John/Joan case.
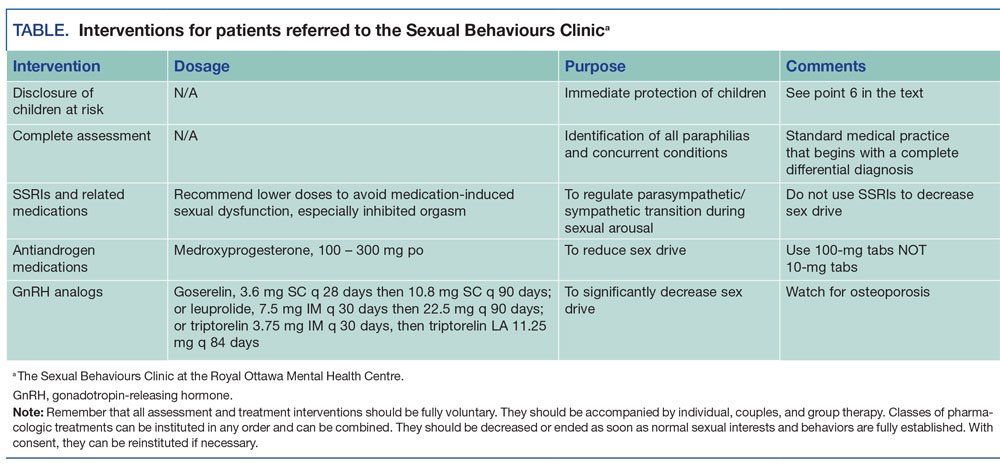
The journal article makes the point that the longer a high-risk sex offender goes without reoffending the less likely he/she is to reoffend. I should also note that the author, J. Paul Fedoroff, MD, is the director of the institution claiming to have successfully treated pædophiles, the Sexual Behaviours Clinic in Ontario, Canada.
This recent BBC radio production called “Can sex offenders and violent criminals be rehabilitated in prison?” (full transcript available here (pdf); the show itself can be listened to online or downloaded as a podcast,) looks at prison treatment programmes for sex offenders (not just CSOs, though they’re included) and violent criminals; the conclusion the presenters draw is that the programmes offered don’t work (more people reoffend after release if they’ve done the course than if they haven’t) and, in fact, can be counterproductive (a case is presented of a man convicted of multiple armed robbery charges who used the knowledge he gained in the courses to plan and execute more armed robberies after he was released.) One of the CSOs interviewed says that during the courses the participants were required to describe, in great detail, their assaults, and said that some of the pædophiles “got off” (his words) on the stories. While the programme was entirely subjective, I found it compelling.
This all seems to raise some serious questions about how we (society) should manage CSOs. If Federoff’s right, the treatment administered by the SBC works; there seems to be a very limited amount of research to support it, and that all seems to have come from the SBC itself. If it does work, though, should it ba offered to convicted pædophile CSOs as a treatment? The BBC programme indicates (actually, it baldly states) that current rehabilitation attempts have no positive outcome, and indeed have negative outcomes, so if Federoff’s treatments do work, it would seem a better option to use those. OTOH, if Cantor’s right, would it be possible to surgically or chemically “rewire” the crossed regions of the brain? Synæsthetes don’t want their condition “cured” (understandably,) so even if Ramachandran’s right there’d be no way of testing those methods with that condition. If Money’s right, and it’s untreatable and immutable, how should we treat pædophile CSOs? Our primary purpose should be to protect children and adults from sexual predation; does that imply that we should keep CSOs in prison for the rest of their life?