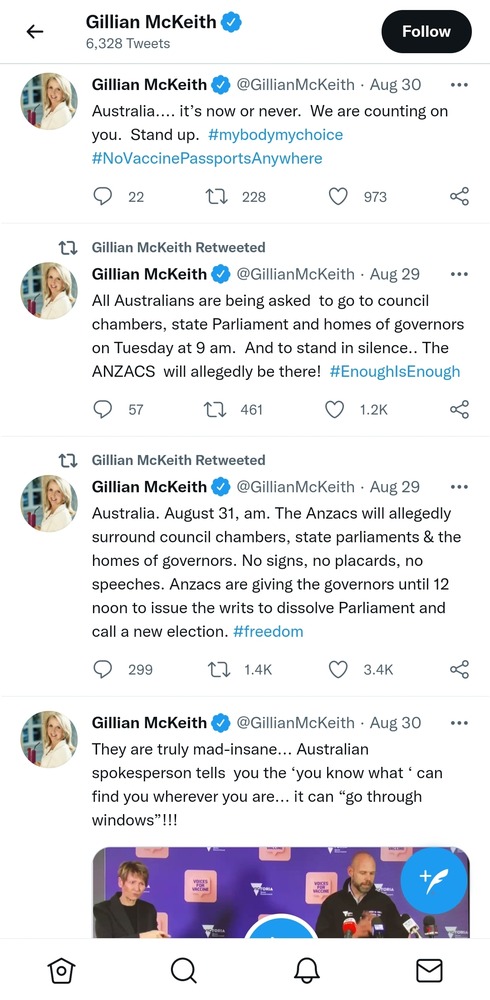
Can someone who knows NSW and has some idea of where is locked down please tell me if these protests are in locked down areas? Or are these people protesting about something that only partly affects them?
Can someone who knows NSW and has some idea of where is locked down please tell me if these protests are in locked down areas? Or are these people protesting about something that only partly affects them?
The whole of NSW is under stay-at-home orders. After they realised COVID had gotten into the Aboriginal population.
Police arrest Australian-born conspiracy theorist Karen Brewer in Kaikohe and Reignite Democracy Australia leader Monica Smit in Melbourne, in separate incidents
Was chatting to the sprogs over dinner, a classic seafood linguine, and they suggested that putting the vaccine into a vaping form and you’d have the 14 to 22 year old cohort covered in a week. I was “what, is it popular?” and they were both “derrr”.
Was chatting to the sprogs over dinner, a classic seafood linguine, and they suggested that putting the vaccine into a vaping form and you’d have the 14 to 22 year old cohort covered in a week. I was “what, is it popular?” and they were both “derrr”.
The things you learn.
Just goes to show the youth are just as stupid these days as we were when we were youths.
I wouldn’t go so far as to call it a nonsense. The issue with the Doherty report is that it’s being treated as a gospel and has become a political tool for politicians who wish to cherry-pick the parts they like and ignore the rest. The report models for a very specific set of circumstances: low caseloads with moderate-to-strong TTIQ, along with recommendations for masks, etc.. Neither of those things (caseloads; TTIQ) are as per the model at present (particularly in NSW; but even the caseload in VIC is too high for the model’s optimal success), and so the model at present isn’t applicable.
If politicians wish to hold true to this model, then they need to work towards creating the environment whereby the model can become reality. Instead, they’ve jumped ahead to the conclusion, and that’s what they’re selling us – several months too early, and with too many cases for the model to be relevant. They’re selling hope to lepers; and eventually, the likes of Berejiklian and Morrison will have to explain why the cases and deaths are heading north when the model said X would happen, but instead Y happened. It’s going to be very hard for them to find a way out of the hole they’ve dug for themselves.
Furthermore, there are other models, some which paint more grim pictures. They’re being conveniently ignored…
So for what it’s worth, the Doherty model is fine, as is the Institute. But the model is no longer relevant, and won’t be until such time as it can be tested against the environment it actually models for.
I wouldn’t go so far as to call it a nonsense. The issue with the Doherty report is that it’s being treated as a gospel and has become a political tool for politicians who wish to cherry-pick the parts they like and ignore the rest. The report models for a very specific set of circumstances: low caseloads with moderate-to-strong TTIQ, along with recommendations for masks, etc.. Neither of those things (caseloads; TTIQ) are as per the model at present (particularly in NSW; but even the caseload in VIC is too high for the model’s optimal success), and so the model at present isn’t applicable.
If politicians wish to hold true to this model, then they need to work towards creating the environment whereby the model can become reality. Instead, they’ve jumped ahead to the conclusion, and that’s what they’re selling us – several months too early, and with too many cases for the model to be relevant. They’re selling hope to lepers; and eventually, the likes of Berejiklian and Morrison will have to explain why the cases and deaths are heading north when the model said X would happen, but instead Y happened. It’s going to be very hard for them to find a way out of the hole they’ve dug for themselves.
Furthermore, there are other models, some which paint more grim pictures. They’re being conveniently ignored…
So for what it’s worth, the Doherty model is fine, as is the Institute. But the model is no longer relevant, and won’t be until such time as it can be tested against the environment it actually models for.
Iirc the model requires about 30 cases a day and highly effective contact tracing, it’ll be months before we’re back to that in the gold standard state.
I wouldn’t go so far as to call it a nonsense. The issue with the Doherty report is that it’s being treated as a gospel and has become a political tool for politicians who wish to cherry-pick the parts they like and ignore the rest. The report models for a very specific set of circumstances: low caseloads with moderate-to-strong TTIQ, along with recommendations for masks, etc.. Neither of those things (caseloads; TTIQ) are as per the model at present (particularly in NSW; but even the caseload in VIC is too high for the model’s optimal success), and so the model at present isn’t applicable.
If politicians wish to hold true to this model, then they need to work towards creating the environment whereby the model can become reality. Instead, they’ve jumped ahead to the conclusion, and that’s what they’re selling us – several months too early, and with too many cases for the model to be relevant. They’re selling hope to lepers; and eventually, the likes of Berejiklian and Morrison will have to explain why the cases and deaths are heading north when the model said X would happen, but instead Y happened. It’s going to be very hard for them to find a way out of the hole they’ve dug for themselves.
Furthermore, there are other models, some which paint more grim pictures. They’re being conveniently ignored…
So for what it’s worth, the Doherty model is fine, as is the Institute. But the model is no longer relevant, and won’t be until such time as it can be tested against the environment it actually models for.
Iirc the model requires about 30 cases a day and highly effective contact tracing, it’ll be months before we’re back to that in the gold standard state.
but as this place is well known for, tell us
how many contributors here actually read Doherty report
and overall yes the comment quoted above does seem to touch on important points we are inclined to agree are valid
Unfortunately that’s just about right. Malta is currently getting significant covid deaths despite being 80% fully vaccinated.
Vaccines can be manufactured that induce herd immunity, but none of the vaccines currently being circulated are of this type.
On the other hand, a 0.1% vaccination level, if the vaccines are given to the right people, is completely effective when combined with border security, as we’ve seen in China. In Australia, the governments are so stupid that we’ve seen a large number of instances where the vaccine has not been given to the right people, the super-spreaders.
Morrison has negotiated a deal with Singapore whereby they will send us 500000 pfizer hits that are going to expire soon. In return we’ll send them 500000 in six months’ time.
Unfortunately that’s just about right. Malta is currently getting significant covid deaths despite being 80% fully vaccinated.
Vaccines can be manufactured that induce herd immunity, but none of the vaccines currently being circulated are of this type.
On the other hand, a 0.1% vaccination level, if the vaccines are given to the right people, is completely effective when combined with border security, as we’ve seen in China. In Australia, the governments are so stupid that we’ve seen a large number of instances where the vaccine has not been given to the right people, the super-spreaders.
It’s called ‘incentivisation’.
To prompt people to go and get their vaccine. You don’t want to be one of the 30% when the floodgate opens, now do you?
And when did it become 70% anyway? All the earlier talk was about 80%. Lobbyists too impatient to wait for that last 10%, perhaps?
Unfortunately that’s just about right. Malta is currently getting significant covid deaths despite being 80% fully vaccinated.
Vaccines can be manufactured that induce herd immunity, but none of the vaccines currently being circulated are of this type.
On the other hand, a 0.1% vaccination level, if the vaccines are given to the right people, is completely effective when combined with border security, as we’ve seen in China. In Australia, the governments are so stupid that we’ve seen a large number of instances where the vaccine has not been given to the right people, the super-spreaders.
>>>>>> In Australia, the governments are so stupid that we’ve seen a large number of instances where the vaccine has not been given to the right people, the super-spreaders.
This requires a reliable method to predict who the super-spreaders are, before they super-spread the virus. Do you know of such a method?
Victoria to start easing lockdown restrictions even though case numbers are rising.
https://www.abc.net.au/news/2021-09-01/victoria-covid-cases-lockdown-melbourne-restrictions/100423686
Covid-19 patients with severe symptoms suffer long-lasting cognitive impairments
Even those who had milder symptoms performed worse on brain-function tests
Aug 31st 2021
Daily Chart
Covid-19 patients with severe symptoms suffer long-lasting cognitive impairments
Even those who had milder symptoms performed worse on brain-function tests
AS VACCINATIONS stem the tide of severe covid-19 cases in the rich world, attention is turning to the virus’s after-effects. Many people experience symptoms after recovery, such as fatigue, sometimes forcing changes in work and lifestyle. Among the least understood aspects of “long covid” are problems with memory and concentration, often known as “brain fog”.
A joint Anglo-American research team set out to measure covid-19’s effect on mental ability, publishing their results in the Lancet EClinicalMedicine. They teamed up with the BBC, Britain’s national broadcaster, on the Great British Intelligence Test, an online assessment billed to the public as a way to “test your cognitive strengths”. Some 80,000 people signed up.
Participants completed several activities assessing cognitive function. They were asked to remember lists of numbers or locations on a chessboard to test their recall. A “Tower of Hanoi”-style game, in which stackable blocks are moved from one pin to another, measured planning capacity. Two tasks assessed verbal skills, while a Tetris-style game assessed problem-solving. The ability to manipulate information was tested by matching identical shapes that had been rotated. To prevent bias, questions about the virus, as well as about demographic factors such as age, ethnicity and socioeconomic status, were asked only after the test had ended.
After controlling for factors including age, sex, educational level, first language and income, people who reported having recovered from covid-19 were found to perform worse than those who thought they had never caught it. The more severe the symptoms, the worse they performed. Those who had been put on a ventilator fared poorest of all. The gap between their average performance and that of participants who reported never having had covid-19 was equivalent to seven IQ points. Those who had been put on a ventilator scored lower than people who reported having a learning disability or had previously had a stroke.
People ventilated for different respiratory diseases often face similar cognitive issues. But the performance of those with mild covid-19 symptoms suffered more than would be expected in the event of mild illness. (Additionally, patients who had actually tested positive for covid-19, rather than merely suspecting they had caught it, suffered from greater cognitive impairment; this is probably because some in the latter camp had misdiagnosed a common cold or throat infection.)
Scientists are still unsure how exactly covid-19 is linked to cognitive impairment. One preprint study compared brain scans done before the pandemic with scans of the same patients taken after they had tested positive. The researchers found that regions of the brain associated with memory, taste and smell had shrunk. There are several theories as to the cause. Some studies argue it is the body’s own immune response causing harm. Others show that the virus specifically attacks astrocytes, the brain’s “support cells”. A final camp claims the damage is caused by a lack of oxygen.
It remains unclear how long brain fog takes to clear, or if it does at all. That makes it difficult to estimate the lasting economic and social impact. And it reinforces worries that the health effects of covid-19 will linger long after the pandemic is tamed
“Scientists in South Africa are monitoring a new coronavirus variant with an unusually high mutation rate, and whose frequency has gradually increased in recent months, the National Institute for Communicable Diseases said Monday.”
“We have thrown everything at this, but it is now clear to us that we here not going to drive these numbers down.
“They’re instead going to increase.
“Now it’s up to us to make sure they don’t increase too fast and they don’t increase too much relative to the number of people who are getting vaccinated every single day every single week.”
have me a listen and read, see if the modelling included the probable effect that vaccinated people (fully or partially) potentially carry and transmit the virus with impunity, shades of, are likely to get less scrutiny (that lends to testing and more), and that the general idea of being ‘immune’ or vaccination (even availability) lends to similar
“Authorities had expressed optimism about the outbreak’s stability at the start of the week, but Mr Andrews said since then, a deterioration had led to changed public health advice.
The Premier said the state could no longer “hold out hope” that case numbers would fall and must instead focus on suppressing the outbreak’s growth while racing to reach higher vaccination coverage.”
“Authorities had expressed optimism about the outbreak’s stability at the start of the week, but Mr Andrews said since then, a deterioration had led to changed public health advice.
The Premier said the state could no longer “hold out hope” that case numbers would fall and must instead focus on suppressing the outbreak’s growth while racing to reach higher vaccination coverage.”
“Authorities had expressed optimism about the outbreak’s stability at the start of the week, but Mr Andrews said since then, a deterioration had led to changed public health advice.
The Premier said the state could no longer “hold out hope” that case numbers would fall and must instead focus on suppressing the outbreak’s growth while racing to reach higher vaccination coverage.”
With 10 times fewer daily cases, Dan will not be following the example of Gladys, but striving to achieve far better than the NSW disaster.
“Authorities had expressed optimism about the outbreak’s stability at the start of the week, but Mr Andrews said since then, a deterioration had led to changed public health advice.
The Premier said the state could no longer “hold out hope” that case numbers would fall and must instead focus on suppressing the outbreak’s growth while racing to reach higher vaccination coverage.”
“Authorities had expressed optimism about the outbreak’s stability at the start of the week, but Mr Andrews said since then, a deterioration had led to changed public health advice.
The Premier said the state could no longer “hold out hope” that case numbers would fall and must instead focus on suppressing the outbreak’s growth while racing to reach higher vaccination coverage.”
Pity NSW infected Vic in the first place.
Yes, so far the other states Qld WA Tas and SA are keeping it at bay, long may that continue but I’d really like to go up to the Redoubt in the not too distant future.
“Authorities had expressed optimism about the outbreak’s stability at the start of the week, but Mr Andrews said since then, a deterioration had led to changed public health advice.
The Premier said the state could no longer “hold out hope” that case numbers would fall and must instead focus on suppressing the outbreak’s growth while racing to reach higher vaccination coverage.”
Pity NSW infected Vic in the first place.
Yes, so far the other states Qld WA Tas and SA are keeping it at bay, long may that continue but I’d really like to go up to the Redoubt in the not too distant future.
Yes, so far the other states Qld WA Tas and SA are keeping it at bay, long may that continue but I’d really like to go up to the Redoubt in the not too distant future.
Do your cattle need checking?
None on there at the moment but even if there were I’d still have to do home quarantine for two weeks.
It’s the rule now even if you’ve got a pass.
Yes, so far the other states Qld WA Tas and SA are keeping it at bay, long may that continue but I’d really like to go up to the Redoubt in the not too distant future.
Do your cattle need checking?
None on there at the moment but even if there were I’d still have to do home quarantine for two weeks.
It’s the rule now even if you’ve got a pass.
Yes, so far the other states Qld WA Tas and SA are keeping it at bay, long may that continue but I’d really like to go up to the Redoubt in the not too distant future.
Do your cattle need checking?
None on there at the moment but even if there were I’d still have to do home quarantine for two weeks.
It’s the rule now even if you’ve got a pass.
I couldn’t find the fine detail of our rules here, although I did know that previously we were allowed to go and get firewood outside our 5km radius etc. So today we decided to take the slasher up anyway because we really do have to do some fuel reduction/fire danger mitigation work at this time of year if we want to protect the shed even a little bit for the Summer. I cleared a bit more bracken off the fenceline, and around the shed, and Mr buffy ran the Razorback around some of the access tracks. In case we were stopped on the way back we did throw a few bits of wood into the trailer. And I carried a copy of the rates notice for the block, where it is categorized as primary industry. Going over we didn’t go into any towns, although coming back we called at the supermarket for some meat for tea. No border crossing involved, so no quarantine involved for us.
None on there at the moment but even if there were I’d still have to do home quarantine for two weeks.
It’s the rule now even if you’ve got a pass.
I couldn’t find the fine detail of our rules here, although I did know that previously we were allowed to go and get firewood outside our 5km radius etc. So today we decided to take the slasher up anyway because we really do have to do some fuel reduction/fire danger mitigation work at this time of year if we want to protect the shed even a little bit for the Summer. I cleared a bit more bracken off the fenceline, and around the shed, and Mr buffy ran the Razorback around some of the access tracks. In case we were stopped on the way back we did throw a few bits of wood into the trailer. And I carried a copy of the rates notice for the block, where it is categorized as primary industry. Going over we didn’t go into any towns, although coming back we called at the supermarket for some meat for tea. No border crossing involved, so no quarantine involved for us.
The census lady dropped in to pick up the form today. No sign of a mask. She said she had 80 houses to visit.
Feds should have had this sort of thing going from the start. Mobile caravan setups visiting small towns and going around the suburbs. My dentist and I had this discussion last week.
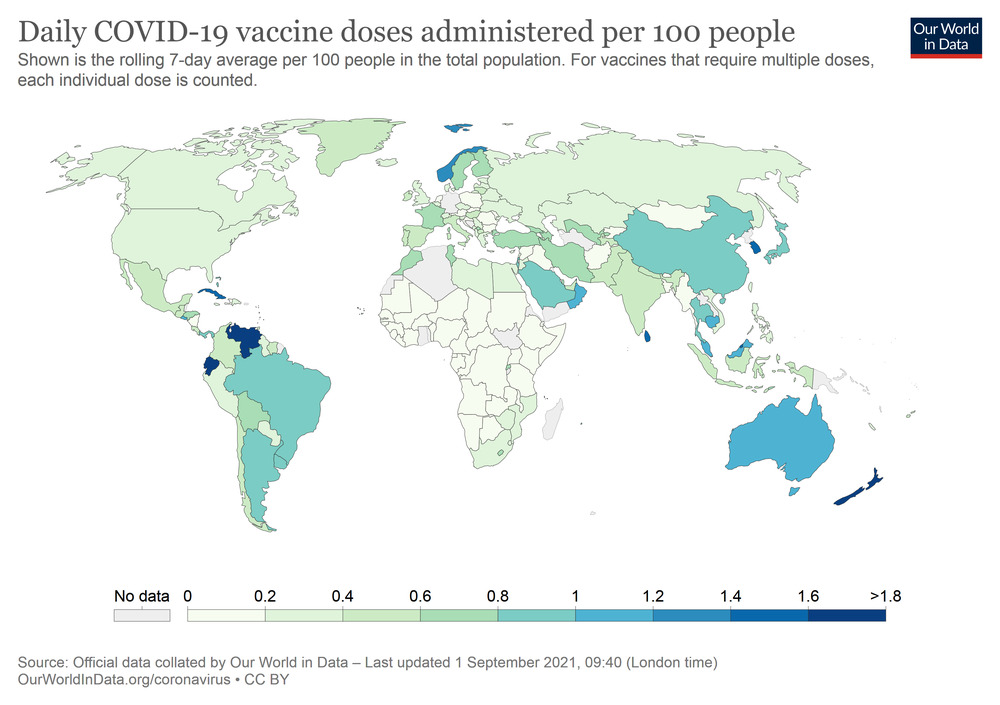
Australia has one of the highest daily vaccination rates per capita in the world.
At the top of the leader board is (7 day smoothed) is Ecuador then New Zealand at 1.65% of population per day.
Then Venezuela, Brunei, Korea, Sri Lanka, Cuba, Noirway, Cambodia, El Salvador, Malaysia
Then Australia at 12th in the world with 1.06% of the population per day.
12th for vaccination speed out of 195 or so countries is prtetty darn good.
We ousted Japan recently, Japan used to be ahead of Australia in vaccination speed but has dropped back to 14th in the world.
Daily Chart
Covid-19 patients with severe symptoms suffer long-lasting cognitive impairments
Even those who had milder symptoms performed worse on brain-function tests
AS VACCINATIONS stem the tide of severe covid-19 cases in the rich world, attention is turning to the virus’s after-effects. Many people experience symptoms after recovery, such as fatigue, sometimes forcing changes in work and lifestyle. Among the least understood aspects of “long covid” are problems with memory and concentration, often known as “brain fog”.
A joint Anglo-American research team set out to measure covid-19’s effect on mental ability, publishing their results in the Lancet EClinicalMedicine. They teamed up with the BBC, Britain’s national broadcaster, on the Great British Intelligence Test, an online assessment billed to the public as a way to “test your cognitive strengths”. Some 80,000 people signed up.
Participants completed several activities assessing cognitive function. They were asked to remember lists of numbers or locations on a chessboard to test their recall. A “Tower of Hanoi”-style game, in which stackable blocks are moved from one pin to another, measured planning capacity. Two tasks assessed verbal skills, while a Tetris-style game assessed problem-solving. The ability to manipulate information was tested by matching identical shapes that had been rotated. To prevent bias, questions about the virus, as well as about demographic factors such as age, ethnicity and socioeconomic status, were asked only after the test had ended.
After controlling for factors including age, sex, educational level, first language and income, people who reported having recovered from covid-19 were found to perform worse than those who thought they had never caught it. The more severe the symptoms, the worse they performed. Those who had been put on a ventilator fared poorest of all. The gap between their average performance and that of participants who reported never having had covid-19 was equivalent to seven IQ points. Those who had been put on a ventilator scored lower than people who reported having a learning disability or had previously had a stroke.
People ventilated for different respiratory diseases often face similar cognitive issues. But the performance of those with mild covid-19 symptoms suffered more than would be expected in the event of mild illness. (Additionally, patients who had actually tested positive for covid-19, rather than merely suspecting they had caught it, suffered from greater cognitive impairment; this is probably because some in the latter camp had misdiagnosed a common cold or throat infection.)
Scientists are still unsure how exactly covid-19 is linked to cognitive impairment. One preprint study compared brain scans done before the pandemic with scans of the same patients taken after they had tested positive. The researchers found that regions of the brain associated with memory, taste and smell had shrunk. There are several theories as to the cause. Some studies argue it is the body’s own immune response causing harm. Others show that the virus specifically attacks astrocytes, the brain’s “support cells”. A final camp claims the damage is caused by a lack of oxygen.
It remains unclear how long brain fog takes to clear, or if it does at all. That makes it difficult to estimate the lasting economic and social impact. And it reinforces worries that the health effects of covid-19 will linger long after the pandemic is tamed
wait so does everyone agree now that death is merely the most visible part of the COVID-19 iceberg and that despite this the psychopathic right wing governments all over the world are intent on ramming iceberg at full pace
“We have thrown everything at this, but it is now clear to us that we here not going to drive these numbers down.
“They’re instead going to increase.
“Now it’s up to us to make sure they don’t increase too fast and they don’t increase too much relative to the number of people who are getting vaccinated every single day every single week.”
“Authorities had expressed optimism about the outbreak’s stability at the start of the week, but Mr Andrews said since then, a deterioration had led to changed public health advice.
The Premier said the state could no longer “hold out hope” that case numbers would fall and must instead focus on suppressing the outbreak’s growth while racing to reach higher vaccination coverage.”
So it is a race.
Pity NSW infected Vic in the first place.
Well actually…
vaccinate its way out of the COVID problems. Bummer.
Vaccination is entirely a viable part of most strategies (from “Let It Rip™ at least only 500000 people die instead of 5000000” through to eradication).
The Premier said the state could no longer “hold out hope” that case numbers would fall and must instead focus on suppressing the outbreak’s growth while racing to reach higher vaccination coverage.
As someone mentioned, holding it to lower cases to begin with will mean easier return to 0 when coverage is greater.
have me a listen and read, see if the modelling included the probable effect that vaccinated people (fully or partially) potentially carry and transmit the virus with impunity, shades of, are likely to get less scrutiny (that lends to testing and more), and that the general idea of being ‘immune’ or vaccination (even availability) lends to similar
Our question still stands, did anyone else here read it¿
Covid-19 patients with severe symptoms suffer long-lasting cognitive impairments
Even those who had milder symptoms performed worse on brain-function tests
Participants completed several activities assessing cognitive function. They were asked to remember lists of numbers or locations on a chessboard to test their recall. A “Tower of Hanoi”-style game, in which stackable blocks are moved from one pin to another, measured planning capacity. Two tasks assessed verbal skills, while a Tetris-style game assessed problem-solving. The ability to manipulate information was tested by matching identical shapes that had been rotated. To prevent bias, questions about the virus, as well as about demographic factors such as age, ethnicity and socioeconomic status, were asked only after the test had ended.
After controlling for factors including age, sex, educational level, first language and income, people who reported having recovered from covid-19 were found to perform worse than those who thought they had never caught it. The more severe the symptoms, the worse they performed. Those who had been put on a ventilator fared poorest of all. The gap between their average performance and that of participants who reported never having had covid-19 was equivalent to seven IQ points. Those who had been put on a ventilator scored lower than people who reported having a learning disability or had previously had a stroke.
wait so does everyone agree now that death is merely the most visible part of the COVID-19 iceberg and that despite this the psychopathic right wing governments all over the world are intent on ramming iceberg at full pace
The ongoing Covid-19 pandemic could cause a significant rise in the number of dementia patients in the long term, said the Alzheimer’s Disease International.
Some research has shown that Covid infections can increase a person’s likelihood of developing dementia and cause dementia symptoms to show up earlier, the group said.
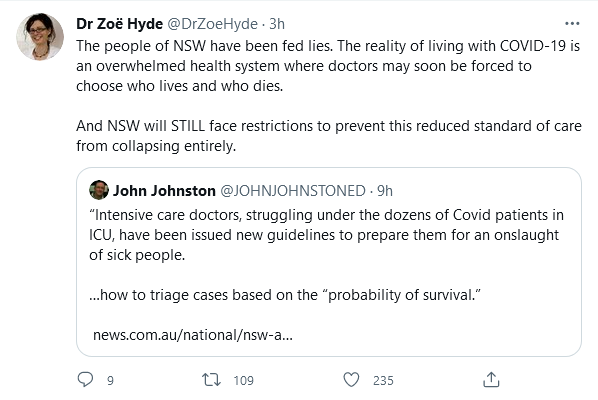
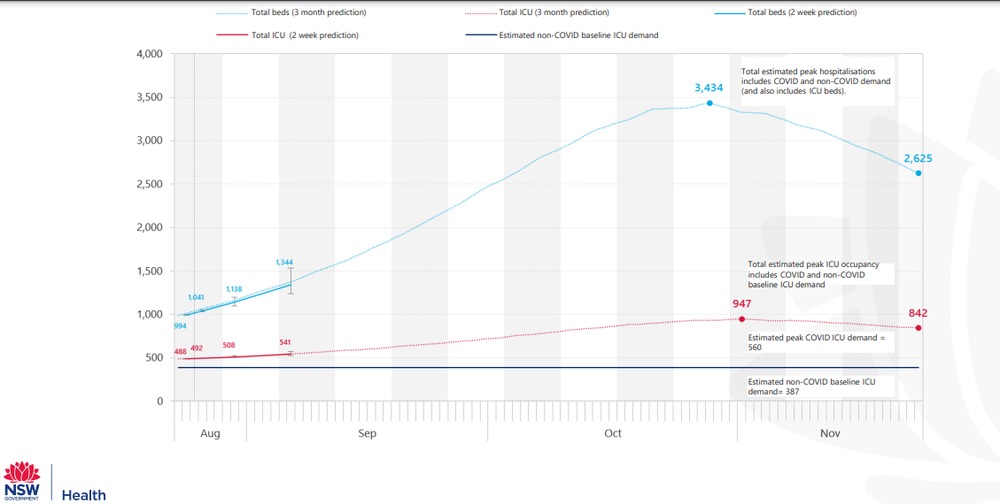
Premier Gladys Berejiklian warned hospitals would feel the full brunt of the rising case numbers in October when more pressure would be placed on intensive care units.
“We will we need to manage things differently,” Ms Berejiklian said.
“We’re in the middle of a pandemic, of course, but will we cope? Of course, we will.”
—
it’s called triage oh yes
read that and a few others, the good work of my favorite broadcaster, seeding the dominoes of covid liberation
Triage in the modern hospital system involves prioritising treatment.
Triage in the COVID era involves deciding who is going to die.
Unfortunately, voters aren’t likely to remember who’s to blame for it when the time comes.
And Labor, especially in NSW, is unlikely to give them any reason to remember.
but honestly, we’re sure that even in “normal” times the choosing and prioritising happens (or you’d have nearly infinite numbers of patients who “might recover” just sitting on ventilators all century), which means that
the health system is always going to be “coping” with whatever is happening, because it will always be delivering whatever it is able to deliver, and what it can’t deliver will be an active choice to prioritise something else
deaths are just numbers so unless someone out there can tell us what number of deaths is “not coping” then we can continue coping
have me a listen and read, see if the modelling included the probable effect that vaccinated people (fully or partially) potentially carry and transmit the virus with impunity, shades of, are likely to get less scrutiny (that lends to testing and more), and that the general idea of being ‘immune’ or vaccination (even availability) lends to similar
Our question still stands, did anyone else here read it¿
have me a listen and read, see if the modelling included the probable effect that vaccinated people (fully or partially) potentially carry and transmit the virus with impunity, shades of, are likely to get less scrutiny (that lends to testing and more), and that the general idea of being ‘immune’ or vaccination (even availability) lends to similar
Our question still stands, did anyone else here read it¿
to other things, get back to that later, it does have me wondering about if I wrote something up to roll out the contagion, deliver it back to nature, what it would read like
NSW health authorities have issued a warning after a COVID-positive person turned up at a Western Sydney hospital ill after overdosing on an anti-parasitic medication and other supposed COVID-19 “cures” ordered online.
Western Sydney Local Health District said a person with COVID-19 presented to Westmead Hospital’s emergency department vomiting and with diarrhoea.
The symptoms weren’t as a result of the virus, but from an overdose of the drug Ivermectin and other medications sold online as “COVID cures”.
Hospital toxicologist Naren Gunja said Ivermectin was an anti-parasitic medication mainly used for farm animals.
He said the person was lucky not to have developed severe toxicity.
“There’s no evidence to support the use of Ivermectin to treat COVID-19,” he said.
“Don’t look for magic cures online, and don’t rely on what’s being peddled on the internet, because none of them work.”
He said others had also turned up at the hospital recently needing treatment after taking a range of dangerous substances to treat COVID-19 including disinfectants, bleach and alcohols.
NSW health authorities have issued a warning after a COVID-positive person turned up at a Western Sydney hospital ill after overdosing on an anti-parasitic medication and other supposed COVID-19 “cures” ordered online.
Western Sydney Local Health District said a person with COVID-19 presented to Westmead Hospital’s emergency department vomiting and with diarrhoea.
The symptoms weren’t as a result of the virus, but from an overdose of the drug Ivermectin and other medications sold online as “COVID cures”.
Hospital toxicologist Naren Gunja said Ivermectin was an anti-parasitic medication mainly used for farm animals.
He said the person was lucky not to have developed severe toxicity.
“There’s no evidence to support the use of Ivermectin to treat COVID-19,” he said.
“Don’t look for magic cures online, and don’t rely on what’s being peddled on the internet, because none of them work.”
He said others had also turned up at the hospital recently needing treatment after taking a range of dangerous substances to treat COVID-19 including disinfectants, bleach and alcohols.
>>Dr Chant says “clearly the advice is that within six weeks of an infection you’re unlikely to be re-infected with Delta”.
She says however, that “natural immunity to Delta or any virus is less effective than a vaccine in terms of long-term immunity”.<<
From the ABC live updates: https://www.abc.net.au/news/2021-09-02/covid-blog-thursday-september-2-australia-vaccines/100423760
Anyone got any idea where this comes from? Why would immunity derived from infection be less effective than immunity from vaccination? I don’t think the Delta version has been around long enough to really know whether immunity to it is long term or not. I haven’t looked particularly hard, but the bits of research I’ve seen reported suggest immunity after infection (or at least antibodies in the blood) lasts months and months, possibly years. (Although again, it’s a bit early at 18 months since ground zero to know much about the long term)
>>Dr Chant says “clearly the advice is that within six weeks of an infection you’re unlikely to be re-infected with Delta”.
She says however, that “natural immunity to Delta or any virus is less effective than a vaccine in terms of long-term immunity”.<<
From the ABC live updates: https://www.abc.net.au/news/2021-09-02/covid-blog-thursday-september-2-australia-vaccines/100423760
Anyone got any idea where this comes from? Why would immunity derived from infection be less effective than immunity from vaccination? I don’t think the Delta version has been around long enough to really know whether immunity to it is long term or not. I haven’t looked particularly hard, but the bits of research I’ve seen reported suggest immunity after infection (or at least antibodies in the blood) lasts months and months, possibly years. (Although again, it’s a bit early at 18 months since ground zero to know much about the long term)
I read somewhere in the last few days that the opposite was case. The immunity derived from infection was higher; I just cannot remember where i saw this.
>>Dr Chant says “clearly the advice is that within six weeks of an infection you’re unlikely to be re-infected with Delta”.
She says however, that “natural immunity to Delta or any virus is less effective than a vaccine in terms of long-term immunity”.<<
From the ABC live updates: https://www.abc.net.au/news/2021-09-02/covid-blog-thursday-september-2-australia-vaccines/100423760
Anyone got any idea where this comes from? Why would immunity derived from infection be less effective than immunity from vaccination? I don’t think the Delta version has been around long enough to really know whether immunity to it is long term or not. I haven’t looked particularly hard, but the bits of research I’ve seen reported suggest immunity after infection (or at least antibodies in the blood) lasts months and months, possibly years. (Although again, it’s a bit early at 18 months since ground zero to know much about the long term)
I read somewhere in the last few days that the opposite was case. The immunity derived from infection was higher; I just cannot remember where i saw this.
>>Dr Chant says “clearly the advice is that within six weeks of an infection you’re unlikely to be re-infected with Delta”.
She says however, that “natural immunity to Delta or any virus is less effective than a vaccine in terms of long-term immunity”.<<
From the ABC live updates: https://www.abc.net.au/news/2021-09-02/covid-blog-thursday-september-2-australia-vaccines/100423760
Anyone got any idea where this comes from? Why would immunity derived from infection be less effective than immunity from vaccination? I don’t think the Delta version has been around long enough to really know whether immunity to it is long term or not. I haven’t looked particularly hard, but the bits of research I’ve seen reported suggest immunity after infection (or at least antibodies in the blood) lasts months and months, possibly years. (Although again, it’s a bit early at 18 months since ground zero to know much about the long term)
I read somewhere in the last few days that the opposite was case. The immunity derived from infection was higher; I just cannot remember where i saw this.
>>Dr Chant says “clearly the advice is that within six weeks of an infection you’re unlikely to be re-infected with Delta”.
She says however, that “natural immunity to Delta or any virus is less effective than a vaccine in terms of long-term immunity”.<<
From the ABC live updates: https://www.abc.net.au/news/2021-09-02/covid-blog-thursday-september-2-australia-vaccines/100423760
Anyone got any idea where this comes from? Why would immunity derived from infection be less effective than immunity from vaccination? I don’t think the Delta version has been around long enough to really know whether immunity to it is long term or not. I haven’t looked particularly hard, but the bits of research I’ve seen reported suggest immunity after infection (or at least antibodies in the blood) lasts months and months, possibly years. (Although again, it’s a bit early at 18 months since ground zero to know much about the long term)
maybe of the statistical comparison, of the two groups, they adjusted for people that died (and those that became seriously ill and lived), factored those things in, I mean people that stop living have a fairly obvious cessation and absence of immunity, a complete loss of homeostasis, followed by a smell if you don’t get them in the fridge soon enough
perhaps they added those people that attended the funeral also, who knows when you get information about a contagion from anyone in the contagion business, it could be creative license by the broadcaster, I couldn’t say
>>Dr Chant says “clearly the advice is that within six weeks of an infection you’re unlikely to be re-infected with Delta”.
She says however, that “natural immunity to Delta or any virus is less effective than a vaccine in terms of long-term immunity”.<<
From the ABC live updates: https://www.abc.net.au/news/2021-09-02/covid-blog-thursday-september-2-australia-vaccines/100423760
Anyone got any idea where this comes from? Why would immunity derived from infection be less effective than immunity from vaccination? I don’t think the Delta version has been around long enough to really know whether immunity to it is long term or not. I haven’t looked particularly hard, but the bits of research I’ve seen reported suggest immunity after infection (or at least antibodies in the blood) lasts months and months, possibly years. (Although again, it’s a bit early at 18 months since ground zero to know much about the long term)
maybe of the statistical comparison, of the two groups, they adjusted for people that died (and those that became seriously ill and lived), factored those things in, I mean people that stop living have a fairly obvious cessation and absence of immunity, a complete loss of homeostasis, followed by a smell if you don’t get them in the fridge soon enough
perhaps they added those people that attended the funeral also, who knows when you get information about a contagion from anyone in the contagion business, it could be creative license by the broadcaster, I couldn’t say
Either way, if you do have antibodies still persisting wouldn’t subsequent infections be less severe and create antibodies?
Recent news about Ivermectin reminded me to check where the research is up to.
Cochrane Review:
“Based on the current very low‐ to low‐certainty evidence, we are uncertain about the efficacy and safety of ivermectin used to treat or prevent COVID‐19. The completed studies are small and few are considered high quality. Several studies are underway that may produce clearer answers in review updates. Overall, the reliable evidence available does not support the use of ivermectin for treatment or prevention of COVID‐19 outside of well‐designed randomized trials. “
More detail at: https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD015017.pub2/full
Within 4 weeks following infection, 90-99% of individuals infected with the SARS-CoV-2 virus develop detectable neutralizing antibodies.
• The strength and duration of the immune responses to SARS-CoV-2 are not completely understood and currently available data suggests that it varies by age and the severity of symptoms. Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months).
• Some variant SARS-CoV-2 viruses with key changes in the spike protein have a reduced susceptibility to neutralization by antibodies in the blood. While neutralizing antibodies mainly target the spike protein, cellular immunity elicited by natural infection also target other viral proteins, which tend to be more conserved across variants than the spike protein. The ability of emerging virus variants (variants of interest and variants of concern) to evade immune responses is under investigation by researchers around the world.
• There are many available serologic assays that measure the antibody response to SARS-CoV-2 infection, but at the present time, the correlates of protection are not well understood.
Within 4 weeks following infection, 90-99% of individuals infected with the SARS-CoV-2 virus develop detectable neutralizing antibodies.
• The strength and duration of the immune responses to SARS-CoV-2 are not completely understood and currently available data suggests that it varies by age and the severity of symptoms. Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months).
• Some variant SARS-CoV-2 viruses with key changes in the spike protein have a reduced susceptibility to neutralization by antibodies in the blood. While neutralizing antibodies mainly target the spike protein, cellular immunity elicited by natural infection also target other viral proteins, which tend to be more conserved across variants than the spike protein. The ability of emerging virus variants (variants of interest and variants of concern) to evade immune responses is under investigation by researchers around the world.
• There are many available serologic assays that measure the antibody response to SARS-CoV-2 infection, but at the present time, the correlates of protection are not well understood.
Within 4 weeks following infection, 90-99% of individuals infected with the SARS-CoV-2 virus develop detectable neutralizing antibodies.
• The strength and duration of the immune responses to SARS-CoV-2 are not completely understood and currently available data suggests that it varies by age and the severity of symptoms. Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months).
• Some variant SARS-CoV-2 viruses with key changes in the spike protein have a reduced susceptibility to neutralization by antibodies in the blood. While neutralizing antibodies mainly target the spike protein, cellular immunity elicited by natural infection also target other viral proteins, which tend to be more conserved across variants than the spike protein. The ability of emerging virus variants (variants of interest and variants of concern) to evade immune responses is under investigation by researchers around the world.
• There are many available serologic assays that measure the antibody response to SARS-CoV-2 infection, but at the present time, the correlates of protection are not well understood.
Well it is a neo or new virus.
Not sure how that is relevent. We were earlier discussing a statement by Kerry Chant that
“She says however, that “natural immunity to Delta or any virus is less effective than a vaccine in terms of long-term immunity”.
and wondering how this could possibly be known. I call shenanigans on that statement.
Within 4 weeks following infection, 90-99% of individuals infected with the SARS-CoV-2 virus develop detectable neutralizing antibodies.
• The strength and duration of the immune responses to SARS-CoV-2 are not completely understood and currently available data suggests that it varies by age and the severity of symptoms. Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months).
• Some variant SARS-CoV-2 viruses with key changes in the spike protein have a reduced susceptibility to neutralization by antibodies in the blood. While neutralizing antibodies mainly target the spike protein, cellular immunity elicited by natural infection also target other viral proteins, which tend to be more conserved across variants than the spike protein. The ability of emerging virus variants (variants of interest and variants of concern) to evade immune responses is under investigation by researchers around the world.
• There are many available serologic assays that measure the antibody response to SARS-CoV-2 infection, but at the present time, the correlates of protection are not well understood.
Well it is a neo or new virus.
Not sure how that is relevent. We were earlier discussing a statement by Kerry Chant that
“She says however, that “natural immunity to Delta or any virus is less effective than a vaccine in terms of long-term immunity”.
and wondering how this could possibly be known. I call shenanigans on that statement.
In Other News, Authorities Slow Automobiles Down From Their Efficiency Points Ostensibly To Improve Air Quality, Despite Failing To Control An Airborne Pandemic
The French authorities hope that the city of Paris will witness a safer, less dirty, and quieter environment as the new speed limit for drivers comes into effect. “This is not an anti-car measure,” said David Belliard, the deputy Mayor.
“The city wants to encourage walking, cycling, and use of public transport. The new speed limit should help reduce pollution, noise, and the number of serious accidents,” he added.
see some idiocy in there, has no fucken idea how inevitability lends to ideology, is a device of ideology
consider the conceptual poverty in failing to see that WA might rather have covid inevitably later than sooner, even postpone the inevitability into non-existence
dickheads in the contagion business, as if covid is their friend
TRAFFICLIGHTS
David Walsh | Posted on September 2, 2021
Memo from David Walsh to staff, about vaccination at Mona, 2 September 2021
A society with unlimited rights is incapable of standing to adversity.
—Alexander Solzhenitsyn
What happens when we want to undertake a journey, but a government-mandated intervention delays it, because, they say, it serves the greater good? Is that an infringement on our rights?
I’m talking about traffic lights. Today, while taking the kids to school, I had to wait for a total of six minutes while cars went somewhere else. Of course I could have ignored those dastardly traffic lights, but ignoring them, potentially, has consequences. I might get in trouble with the very authorities that I’m resisting. Is running those lights a legitimate protest? Perhaps I should protest by making things worse (I could stand in the middle of the intersection, at great risk to myself to enhance the risk to others—that’d work). I might kill myself. But I’ve got a fancy car that’ll protect me. Perhaps I should run those lights, window down, arm out, middle finger extended. But if I run those lights, others might suffer. Most times, though, I’ll get through unscathed, and cause no diminishment to others. Am I feeling lucky, punk? And anyway, aren’t we a bunch of self-interested, greed-is-good, motherfucking capitalists? Why should I look after others?
But I stopped at the red lights. So did everybody else. If traffic lights are a part of a global conspiracy to turn us all into pawns of the government, or Bill Gates, or 5G, then I’m a government tool. Or just a tool. And so is everybody else.
I’m going to make vaccination mandatory for staff at Mona. If that makes you see red (lights) despite the previous three paragraphs let me, briefly, talk about the nature of risk. Some types of risk are additive (every time you take a bath, there’s a small chance it’ll kill you: but there is no chance it’ll kill anyone else). When you go to work unvaccinated there’s a small chance you’ll get COVID and an even smaller chance you’ll die. But each time you take that risk there is a small chance you’ll kill someone else (it’s multiplicative). That’s not okay. In a perfect world the vaccine would never kill you (a very small risk, but additive, like a bath), and it’d protect you and others completely. It doesn’t give perfect protection. Sometimes traffic lights fail. But we don’t turn them off. That’d kill more people. We keep them on, because mostly, inefficiently and grudgingly, we serve the greater good.
We’ll give you a decent interval to get vaccinated, and if necessary we’ll help you make an appointment.
We used to have co-leaders who could cruise through amber. One has gone to greener pastures (congrats). Patrick will now be our CEO solo. Ably assisted by Liz and Philippa and hundreds of others… you, if you get vaccinated. Patrick has proved he is very wise—these days, he always stops at red lights.
I wrote the above for the staff of Mona. But Emily, who mediates between me and the media, wanted to release it to everyone. ‘Transparency, and anyway, there’ll be leaks, and that’ll cause confusion.’ So I’m telling everyone that’s interested. At Mona we’ll be mandating COVID vaccinations for staff. Most of Mona’s staff are exposed to the public (although, at the moment, we don’t really have a public). Most people who visit Mona are nice, friendly, and respectful. But there’s a small chance that each of them is a reservoir for that beastly COVID virus. I’d like to mandate vaccines for the public, too, but that’d be unfair to, for example, kids. We like kids at Mona. And we like risk at Mona. But we like our staff more.
A few staff might think we are trampling on their rights, but the one right they think we are restricting doesn’t exist. Our staff don’t have the right to trample on the rights of their colleagues. Yes, it’s harsh to deprive someone of their livelihood for the good of others. And it’s harsh to deprive someone of their licence for running red lights. Harsh, but necessary.
TRAFFICLIGHTS
David Walsh | Posted on September 2, 2021
Memo from David Walsh to staff, about vaccination at Mona, 2 September 2021
A society with unlimited rights is incapable of standing to adversity.
—Alexander Solzhenitsyn
What happens when we want to undertake a journey, but a government-mandated intervention delays it, because, they say, it serves the greater good? Is that an infringement on our rights?
I’m talking about traffic lights. Today, while taking the kids to school, I had to wait for a total of six minutes while cars went somewhere else. Of course I could have ignored those dastardly traffic lights, but ignoring them, potentially, has consequences. I might get in trouble with the very authorities that I’m resisting. Is running those lights a legitimate protest? Perhaps I should protest by making things worse (I could stand in the middle of the intersection, at great risk to myself to enhance the risk to others—that’d work). I might kill myself. But I’ve got a fancy car that’ll protect me. Perhaps I should run those lights, window down, arm out, middle finger extended. But if I run those lights, others might suffer. Most times, though, I’ll get through unscathed, and cause no diminishment to others. Am I feeling lucky, punk? And anyway, aren’t we a bunch of self-interested, greed-is-good, motherfucking capitalists? Why should I look after others?
But I stopped at the red lights. So did everybody else. If traffic lights are a part of a global conspiracy to turn us all into pawns of the government, or Bill Gates, or 5G, then I’m a government tool. Or just a tool. And so is everybody else.
I’m going to make vaccination mandatory for staff at Mona. If that makes you see red (lights) despite the previous three paragraphs let me, briefly, talk about the nature of risk. Some types of risk are additive (every time you take a bath, there’s a small chance it’ll kill you: but there is no chance it’ll kill anyone else). When you go to work unvaccinated there’s a small chance you’ll get COVID and an even smaller chance you’ll die. But each time you take that risk there is a small chance you’ll kill someone else (it’s multiplicative). That’s not okay. In a perfect world the vaccine would never kill you (a very small risk, but additive, like a bath), and it’d protect you and others completely. It doesn’t give perfect protection. Sometimes traffic lights fail. But we don’t turn them off. That’d kill more people. We keep them on, because mostly, inefficiently and grudgingly, we serve the greater good.
We’ll give you a decent interval to get vaccinated, and if necessary we’ll help you make an appointment.
We used to have co-leaders who could cruise through amber. One has gone to greener pastures (congrats). Patrick will now be our CEO solo. Ably assisted by Liz and Philippa and hundreds of others… you, if you get vaccinated. Patrick has proved he is very wise—these days, he always stops at red lights.
I wrote the above for the staff of Mona. But Emily, who mediates between me and the media, wanted to release it to everyone. ‘Transparency, and anyway, there’ll be leaks, and that’ll cause confusion.’ So I’m telling everyone that’s interested. At Mona we’ll be mandating COVID vaccinations for staff. Most of Mona’s staff are exposed to the public (although, at the moment, we don’t really have a public). Most people who visit Mona are nice, friendly, and respectful. But there’s a small chance that each of them is a reservoir for that beastly COVID virus. I’d like to mandate vaccines for the public, too, but that’d be unfair to, for example, kids. We like kids at Mona. And we like risk at Mona. But we like our staff more.
A few staff might think we are trampling on their rights, but the one right they think we are restricting doesn’t exist. Our staff don’t have the right to trample on the rights of their colleagues. Yes, it’s harsh to deprive someone of their livelihood for the good of others. And it’s harsh to deprive someone of their licence for running red lights. Harsh, but necessary.
TRAFFICLIGHTS
David Walsh | Posted on September 2, 2021
Memo from David Walsh to staff, about vaccination at Mona, 2 September 2021
A society with unlimited rights is incapable of standing to adversity.
—Alexander Solzhenitsyn
What happens when we want to undertake a journey, but a government-mandated intervention delays it, because, they say, it serves the greater good? Is that an infringement on our rights?
I’m talking about traffic lights. Today, while taking the kids to school, I had to wait for a total of six minutes while cars went somewhere else. Of course I could have ignored those dastardly traffic lights, but ignoring them, potentially, has consequences. I might get in trouble with the very authorities that I’m resisting. Is running those lights a legitimate protest? Perhaps I should protest by making things worse (I could stand in the middle of the intersection, at great risk to myself to enhance the risk to others—that’d work). I might kill myself. But I’ve got a fancy car that’ll protect me. Perhaps I should run those lights, window down, arm out, middle finger extended. But if I run those lights, others might suffer. Most times, though, I’ll get through unscathed, and cause no diminishment to others. Am I feeling lucky, punk? And anyway, aren’t we a bunch of self-interested, greed-is-good, motherfucking capitalists? Why should I look after others?
But I stopped at the red lights. So did everybody else. If traffic lights are a part of a global conspiracy to turn us all into pawns of the government, or Bill Gates, or 5G, then I’m a government tool. Or just a tool. And so is everybody else.
I’m going to make vaccination mandatory for staff at Mona. If that makes you see red (lights) despite the previous three paragraphs let me, briefly, talk about the nature of risk. Some types of risk are additive (every time you take a bath, there’s a small chance it’ll kill you: but there is no chance it’ll kill anyone else). When you go to work unvaccinated there’s a small chance you’ll get COVID and an even smaller chance you’ll die. But each time you take that risk there is a small chance you’ll kill someone else (it’s multiplicative). That’s not okay. In a perfect world the vaccine would never kill you (a very small risk, but additive, like a bath), and it’d protect you and others completely. It doesn’t give perfect protection. Sometimes traffic lights fail. But we don’t turn them off. That’d kill more people. We keep them on, because mostly, inefficiently and grudgingly, we serve the greater good.
We’ll give you a decent interval to get vaccinated, and if necessary we’ll help you make an appointment.
We used to have co-leaders who could cruise through amber. One has gone to greener pastures (congrats). Patrick will now be our CEO solo. Ably assisted by Liz and Philippa and hundreds of others… you, if you get vaccinated. Patrick has proved he is very wise—these days, he always stops at red lights.
I wrote the above for the staff of Mona. But Emily, who mediates between me and the media, wanted to release it to everyone. ‘Transparency, and anyway, there’ll be leaks, and that’ll cause confusion.’ So I’m telling everyone that’s interested. At Mona we’ll be mandating COVID vaccinations for staff. Most of Mona’s staff are exposed to the public (although, at the moment, we don’t really have a public). Most people who visit Mona are nice, friendly, and respectful. But there’s a small chance that each of them is a reservoir for that beastly COVID virus. I’d like to mandate vaccines for the public, too, but that’d be unfair to, for example, kids. We like kids at Mona. And we like risk at Mona. But we like our staff more.
A few staff might think we are trampling on their rights, but the one right they think we are restricting doesn’t exist. Our staff don’t have the right to trample on the rights of their colleagues. Yes, it’s harsh to deprive someone of their livelihood for the good of others. And it’s harsh to deprive someone of their licence for running red lights. Harsh, but necessary.
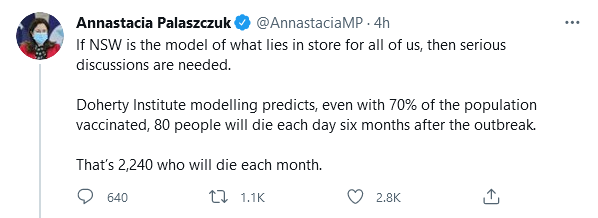
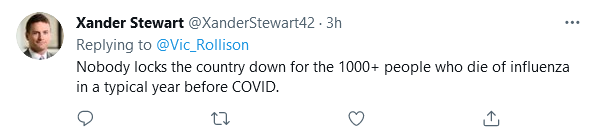
In the last 6 years only one of those had over a 1000 deaths due to the flu. There were 1181 in 2017. For comparison 2016 had 273 deaths.
annastacia is talking daily and monthly
the commonwealth (subject to a questionable international influence) is trying to forge ‘an agreement’ with States, with the assistance of NSWcough, and citizens regard acceptable death totals and death rates, the proposition probably has no legal enforceability because it involves release of a biological hazard (with observed unfriendly mutation potentials), and i’m not even sure the modelling reflects existing realities, or how they would pan out if ‘the plan’ was adopted, or more broadly adopted
TRAFFICLIGHTS
David Walsh | Posted on September 2, 2021
Memo from David Walsh to staff, about vaccination at Mona, 2 September 2021
A society with unlimited rights is incapable of standing to adversity.
—Alexander Solzhenitsyn
What happens when we want to undertake a journey, but a government-mandated intervention delays it, because, they say, it serves the greater good? Is that an infringement on our rights?
I’m talking about traffic lights. Today, while taking the kids to school, I had to wait for a total of six minutes while cars went somewhere else. Of course I could have ignored those dastardly traffic lights, but ignoring them, potentially, has consequences. I might get in trouble with the very authorities that I’m resisting. Is running those lights a legitimate protest? Perhaps I should protest by making things worse (I could stand in the middle of the intersection, at great risk to myself to enhance the risk to others—that’d work). I might kill myself. But I’ve got a fancy car that’ll protect me. Perhaps I should run those lights, window down, arm out, middle finger extended. But if I run those lights, others might suffer. Most times, though, I’ll get through unscathed, and cause no diminishment to others. Am I feeling lucky, punk? And anyway, aren’t we a bunch of self-interested, greed-is-good, motherfucking capitalists? Why should I look after others?
But I stopped at the red lights. So did everybody else. If traffic lights are a part of a global conspiracy to turn us all into pawns of the government, or Bill Gates, or 5G, then I’m a government tool. Or just a tool. And so is everybody else.
I’m going to make vaccination mandatory for staff at Mona. If that makes you see red (lights) despite the previous three paragraphs let me, briefly, talk about the nature of risk. Some types of risk are additive (every time you take a bath, there’s a small chance it’ll kill you: but there is no chance it’ll kill anyone else). When you go to work unvaccinated there’s a small chance you’ll get COVID and an even smaller chance you’ll die. But each time you take that risk there is a small chance you’ll kill someone else (it’s multiplicative). That’s not okay. In a perfect world the vaccine would never kill you (a very small risk, but additive, like a bath), and it’d protect you and others completely. It doesn’t give perfect protection. Sometimes traffic lights fail. But we don’t turn them off. That’d kill more people. We keep them on, because mostly, inefficiently and grudgingly, we serve the greater good.
We’ll give you a decent interval to get vaccinated, and if necessary we’ll help you make an appointment.
We used to have co-leaders who could cruise through amber. One has gone to greener pastures (congrats). Patrick will now be our CEO solo. Ably assisted by Liz and Philippa and hundreds of others… you, if you get vaccinated. Patrick has proved he is very wise—these days, he always stops at red lights.
I wrote the above for the staff of Mona. But Emily, who mediates between me and the media, wanted to release it to everyone. ‘Transparency, and anyway, there’ll be leaks, and that’ll cause confusion.’ So I’m telling everyone that’s interested. At Mona we’ll be mandating COVID vaccinations for staff. Most of Mona’s staff are exposed to the public (although, at the moment, we don’t really have a public). Most people who visit Mona are nice, friendly, and respectful. But there’s a small chance that each of them is a reservoir for that beastly COVID virus. I’d like to mandate vaccines for the public, too, but that’d be unfair to, for example, kids. We like kids at Mona. And we like risk at Mona. But we like our staff more.
A few staff might think we are trampling on their rights, but the one right they think we are restricting doesn’t exist. Our staff don’t have the right to trample on the rights of their colleagues. Yes, it’s harsh to deprive someone of their livelihood for the good of others. And it’s harsh to deprive someone of their licence for running red lights. Harsh, but necessary.
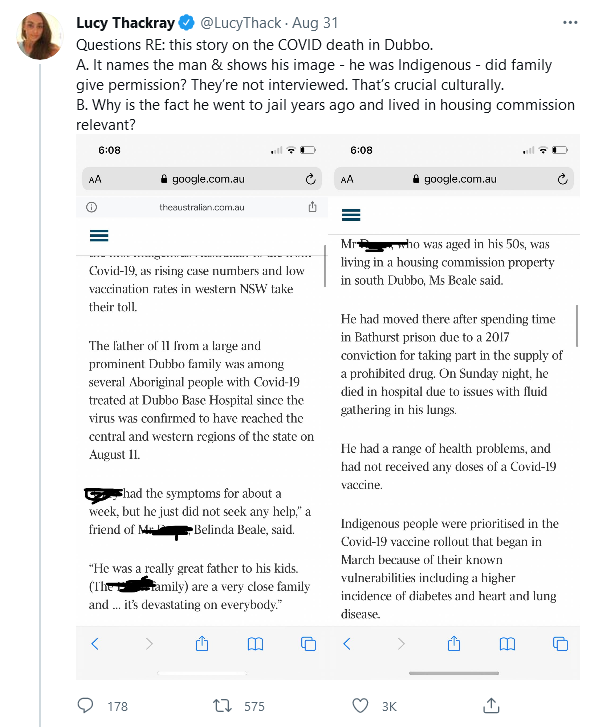
A couple who travelled to Western Sydney and returned to the Central West in early August are believed to have been the region’s first cases.
The Western NSW Local Health District (LHD) said the pair came home a week before the Dubbo and Walgett local government areas were placed into lockdown.
“We do believe we’ve picked up the originating case,” LHD chief executive Scott McLachlan said.
“We believe we’ve tracked that down to a location in Western Sydney that has the same strain of COVID-19, and the biological markers.”
Fragments of the virus had been detected in Dubbo’s sewage before the first case had been identified.
Mr McLachlan said lessons could be drawn from the “spreader” event, but now was not the time to “focus on the rear vision mirror”.
“We’re closer to that original strain but what we now know is there’s so much broad spread of this Delta strain across all of our communities,” Mr McLachlan said.
“It’s not so much about where it came from — it’s about what’s happening today.”
On Thursday the region recorded 23 new cases of COVID-19, nine of which were infectious in the community.
Drug hunt fuels breaches, cops say
The search for drugs has been identified as one possible reason for the spread of the virus in Western NSW.
Police say they have stopped known drug users who do not have a valid excuse to be away from home or who are travelling between towns across the Central West.
The Western Region Commander, Assistant Commissioner Geoff McKechnie said those people were breaching health orders whether or not they had COVID.
“People are driven by their addiction the commercial aspects of it, and their desire to make money by selling drugs,” Assistant Commissioner McKechnie said.
“It still drives that whole industry, so having these health orders in place is not going to totally stamp that out.”
Nonetheless, Assistant Commissioner McKechnie said the lockdown would have disrupted the drug trade.
“I’d be quietly confident that it’s restricted and we saw that in the first round of COVID last year,” he said.
“There certainly was evidence of prices of drugs increasing because of availability, so I think that’s certainly likely that supply has been restricted.”
More than 100 infringement notices have been issued every day this week by police across the Western region, with the majority in Dubbo.
A couple who travelled to Western Sydney and returned to the Central West in early August are believed to have been the region’s first cases.
The Western NSW Local Health District (LHD) said the pair came home a week before the Dubbo and Walgett local government areas were placed into lockdown.
“We do believe we’ve picked up the originating case,” LHD chief executive Scott McLachlan said.
“We believe we’ve tracked that down to a location in Western Sydney that has the same strain of COVID-19, and the biological markers.”
Fragments of the virus had been detected in Dubbo’s sewage before the first case had been identified.
Mr McLachlan said lessons could be drawn from the “spreader” event, but now was not the time to “focus on the rear vision mirror”.
“We’re closer to that original strain but what we now know is there’s so much broad spread of this Delta strain across all of our communities,” Mr McLachlan said.
“It’s not so much about where it came from — it’s about what’s happening today.”
On Thursday the region recorded 23 new cases of COVID-19, nine of which were infectious in the community.
Drug hunt fuels breaches, cops say
The search for drugs has been identified as one possible reason for the spread of the virus in Western NSW.
Police say they have stopped known drug users who do not have a valid excuse to be away from home or who are travelling between towns across the Central West.
The Western Region Commander, Assistant Commissioner Geoff McKechnie said those people were breaching health orders whether or not they had COVID.
“People are driven by their addiction the commercial aspects of it, and their desire to make money by selling drugs,” Assistant Commissioner McKechnie said.
“It still drives that whole industry, so having these health orders in place is not going to totally stamp that out.”
Nonetheless, Assistant Commissioner McKechnie said the lockdown would have disrupted the drug trade.
“I’d be quietly confident that it’s restricted and we saw that in the first round of COVID last year,” he said.
“There certainly was evidence of prices of drugs increasing because of availability, so I think that’s certainly likely that supply has been restricted.”
More than 100 infringement notices have been issued every day this week by police across the Western region, with the majority in Dubbo.
TRAFFICLIGHTS
David Walsh | Posted on September 2, 2021
Memo from David Walsh to staff, about vaccination at Mona, 2 September 2021
A society with unlimited rights is incapable of standing to adversity.
—Alexander Solzhenitsyn
What happens when we want to undertake a journey, but a government-mandated intervention delays it, because, they say, it serves the greater good? Is that an infringement on our rights?
I’m talking about traffic lights. Today, while taking the kids to school, I had to wait for a total of six minutes while cars went somewhere else. Of course I could have ignored those dastardly traffic lights, but ignoring them, potentially, has consequences. I might get in trouble with the very authorities that I’m resisting. Is running those lights a legitimate protest? Perhaps I should protest by making things worse (I could stand in the middle of the intersection, at great risk to myself to enhance the risk to others—that’d work). I might kill myself. But I’ve got a fancy car that’ll protect me. Perhaps I should run those lights, window down, arm out, middle finger extended. But if I run those lights, others might suffer. Most times, though, I’ll get through unscathed, and cause no diminishment to others. Am I feeling lucky, punk? And anyway, aren’t we a bunch of self-interested, greed-is-good, motherfucking capitalists? Why should I look after others?
But I stopped at the red lights. So did everybody else. If traffic lights are a part of a global conspiracy to turn us all into pawns of the government, or Bill Gates, or 5G, then I’m a government tool. Or just a tool. And so is everybody else.
I’m going to make vaccination mandatory for staff at Mona. If that makes you see red (lights) despite the previous three paragraphs let me, briefly, talk about the nature of risk. Some types of risk are additive (every time you take a bath, there’s a small chance it’ll kill you: but there is no chance it’ll kill anyone else). When you go to work unvaccinated there’s a small chance you’ll get COVID and an even smaller chance you’ll die. But each time you take that risk there is a small chance you’ll kill someone else (it’s multiplicative). That’s not okay. In a perfect world the vaccine would never kill you (a very small risk, but additive, like a bath), and it’d protect you and others completely. It doesn’t give perfect protection. Sometimes traffic lights fail. But we don’t turn them off. That’d kill more people. We keep them on, because mostly, inefficiently and grudgingly, we serve the greater good.
We’ll give you a decent interval to get vaccinated, and if necessary we’ll help you make an appointment.
We used to have co-leaders who could cruise through amber. One has gone to greener pastures (congrats). Patrick will now be our CEO solo. Ably assisted by Liz and Philippa and hundreds of others… you, if you get vaccinated. Patrick has proved he is very wise—these days, he always stops at red lights.
I wrote the above for the staff of Mona. But Emily, who mediates between me and the media, wanted to release it to everyone. ‘Transparency, and anyway, there’ll be leaks, and that’ll cause confusion.’ So I’m telling everyone that’s interested. At Mona we’ll be mandating COVID vaccinations for staff. Most of Mona’s staff are exposed to the public (although, at the moment, we don’t really have a public). Most people who visit Mona are nice, friendly, and respectful. But there’s a small chance that each of them is a reservoir for that beastly COVID virus. I’d like to mandate vaccines for the public, too, but that’d be unfair to, for example, kids. We like kids at Mona. And we like risk at Mona. But we like our staff more.
A few staff might think we are trampling on their rights, but the one right they think we are restricting doesn’t exist. Our staff don’t have the right to trample on the rights of their colleagues. Yes, it’s harsh to deprive someone of their livelihood for the good of others. And it’s harsh to deprive someone of their licence for running red lights. Harsh, but necessary.
Nicely put, Mr Walsh.
:)
he’s all about gambling. Buut he is all about winning.
And….Sweden has dropped another slot to number 40 on the chart according to deaths per million. They have now been running at practically zero deaths per day for a couple of months. I didn’t expect Liechtenstein to overtake them yet. Next in line is Latvia and then South Africa.
And….Sweden has dropped another slot to number 40 on the chart according to deaths per million. They have now been running at practically zero deaths per day for a couple of months. I didn’t expect Liechtenstein to overtake them yet. Next in line is Latvia and then South Africa.
And….Sweden has dropped another slot to number 40 on the chart according to deaths per million. They have now been running at practically zero deaths per day for a couple of months. I didn’t expect Liechtenstein to overtake them yet. Next in line is Latvia and then South Africa.
And….Sweden has dropped another slot to number 40 on the chart according to deaths per million. They have now been running at practically zero deaths per day for a couple of months. I didn’t expect Liechtenstein to overtake them yet. Next in line is Latvia and then South Africa.
How changed tack? They now let people come in from other countries, with conditions. Is that what you mean?
I mean since they tightened their restrictions earlier in the year. It marked the start of bringing down the death rate.
What did they change? They seem to have been opening up for quite some time.
Their initial policy was one of mostly voluntary lockdown measures which meant a higher death rate than other Nordic countries. They then as DV said changed tack to a more stricter regime with a corresponding fall in deaths. That they have not had further waves of deaths since does not mean that their initial policy of high death rates and significant economic damage was somehow admirable.
I mean since they tightened their restrictions earlier in the year. It marked the start of bringing down the death rate.
What did they change? They seem to have been opening up for quite some time.
Their initial policy was one of mostly voluntary lockdown measures which meant a higher death rate than other Nordic countries. They then as DV said changed tack to a more stricter regime with a corresponding fall in deaths. That they have not had further waves of deaths since does not mean that their initial policy of high death rates and significant economic damage was somehow admirable.
I mean since they tightened their restrictions earlier in the year. It marked the start of bringing down the death rate.
What did they change? They seem to have been opening up for quite some time.
Their initial policy was one of mostly voluntary lockdown measures which meant a higher death rate than other Nordic countries. They then as DV said changed tack to a more stricter regime with a corresponding fall in deaths. That they have not had further waves of deaths since does not mean that their initial policy of high death rates and significant economic damage was somehow admirable.
There are some differences from other Nordic countries in terms of urbanization, which is relevent as well. And they didn’t change things until after the first wave. Back at the beginning, no-one knew this thing went for the elderly. Unfortunately for them, it does, and it got loose in the nursing homes. I think this happened in the UK as well.
There is a lot of hindsight going on. You need to try to remember that the state of knowledge has changed over time. Remember masks, as an example. You can’t easily judge decisions made on a much much smaller knowledge base on the basis of what we know now. It’s not easy for anyone, it seems such a long time now.
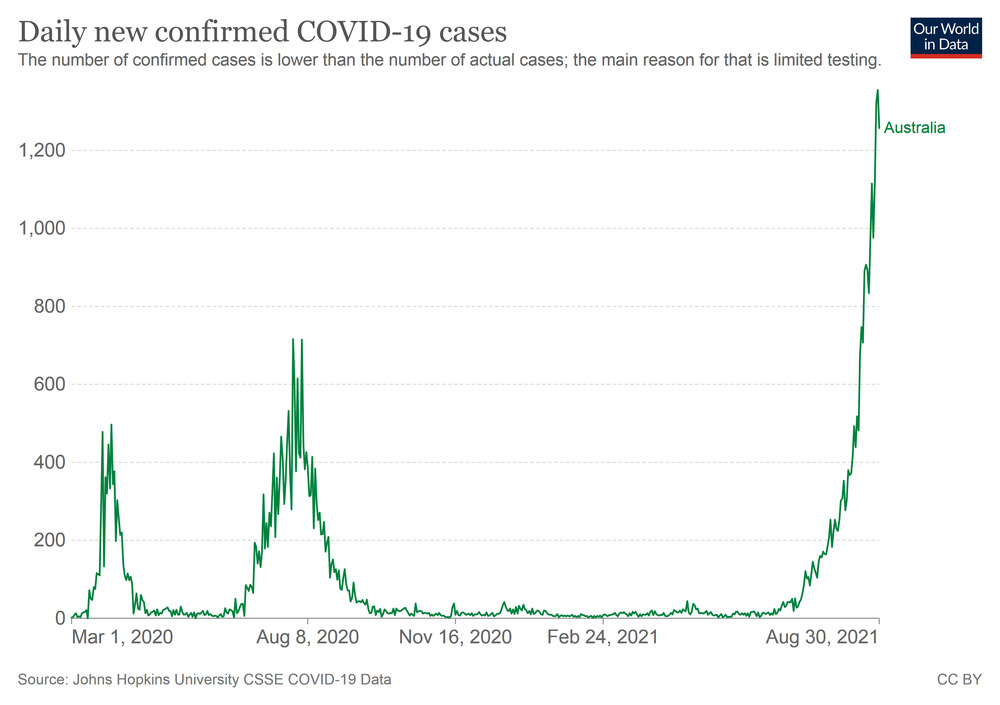
One grim milestone I missed was Australia ticking over to four digits in the deathcount.
Still, doing pretty well overall.
I get the feeling that we ain’t seen nothing yet.
If the Doherty Institute modelling is right, we are looking at something like 2000 a year if we do things right. We probably need to be realistic about this.
Of course this also means maybe 30000 a year who live on with lasting illness of disability. Surviving Covid ain’t always a picnic.
One grim milestone I missed was Australia ticking over to four digits in the deathcount.
Still, doing pretty well overall.
I get the feeling that we ain’t seen nothing yet.
If the Doherty Institute modelling is right, we are looking at something like 2000 a year if we do things right. We probably need to be realistic about this.
Of course this also means maybe 30000 a year who live on with lasting illness of disability. Surviving Covid ain’t always a picnic.
If the Doherty Institute modelling is right, we are looking at something like 2000 a year if we do things right. We probably need to be realistic about this.
Of course this also means maybe 30000 a year who live on with lasting illness of disability. Surviving Covid ain’t always a picnic.
They arent going to follow the modelling.
Shrug if they had gotten it to zero then we could be partying like it’s 1999 year without worrying or restricting except quarantine shrug.
OK, found the stuff about Sweden making new laws. They were passed in January this year. Prior to that their Constitution made it difficult to enforce lockdowns.
If the Doherty Institute modelling is right, we are looking at something like 2000 a year if we do things right. We probably need to be realistic about this.
Of course this also means maybe 30000 a year who live on with lasting illness of disability. Surviving Covid ain’t always a picnic.
They arent going to follow the modelling.
Shrug if they had gotten it to zero then we could be partying like it’s 1999 year without worrying or restricting except quarantine shrug.
What did they change? They seem to have been opening up for quite some time.
Their initial policy was one of mostly voluntary lockdown measures which meant a higher death rate than other Nordic countries. They then as DV said changed tack to a more stricter regime with a corresponding fall in deaths. That they have not had further waves of deaths since does not mean that their initial policy of high death rates and significant economic damage was somehow admirable.
There are some differences from other Nordic countries in terms of urbanization, which is relevent as well. And they didn’t change things until after the first wave. Back at the beginning, no-one knew this thing went for the elderly. Unfortunately for them, it does, and it got loose in the nursing homes. I think this happened in the UK as well.
There is a lot of hindsight going on. You need to try to remember that the state of knowledge has changed over time. Remember masks, as an example. You can’t easily judge decisions made on a much much smaller knowledge base on the basis of what we know now. It’s not easy for anyone, it seems such a long time now.
The Swedes were an outlier from the very beginning when it came to most countries’ policy response.
OK, found the stuff about Sweden making new laws. They were passed in January this year. Prior to that their Constitution made it difficult to enforce lockdowns.
Michael Fumento is a lawyer, author, and journalist who has been writing on epidemic hysterias for 35 years.
…
Enough said.
:)
Oh, and….they aren’t Communists!
;)
AIER, that is.
Founded in 1933, the American Institute for Economic Research (AIER) is one of the oldest and most respected nonpartisan economic research and advocacy organizations in the country. With a global reach and influence, AIER is dedicated to developing and promoting the ideas of pure freedom and private governance by combining advanced economic research with accessible media outreach and educational programming to cultivate a better, broader understanding of the fundamental principles that enable peace and prosperity around the world.
Founded in 1933, the American Institute for Economic Research (AIER) is one of the oldest and most respected nonpartisan economic research and advocacy organizations in the country. With a global reach and influence, AIER is dedicated to developing and promoting the ideas of pure freedom and private governance by combining advanced economic research with accessible media outreach and educational programming to cultivate a better, broader understanding of the fundamental principles that enable peace and prosperity around the world.
Founded in 1933, the American Institute for Economic Research (AIER) is one of the oldest and most respected nonpartisan economic research and advocacy organizations in the country. With a global reach and influence, AIER is dedicated to developing and promoting the ideas of pure freedom and private governance by combining advanced economic research with accessible media outreach and educational programming to cultivate a better, broader understanding of the fundamental principles that enable peace and prosperity around the world.
Which looks like an astounding stat until you look uo that 73% of American adults are obese or overweight.
It’s kind of weird that the article doesn’t include this number, which is crucial to contextualising the news.
However, the article does state the following key point:
Just over 42% of the U.S. population was considered obese in 2018, according to the agency’s most recent statistics. Overweight is defined as having a body mass index of 25 or more, while obesity is defined as having a BMI of 30 or more.
Which looks like an astounding stat until you look uo that 73% of American adults are obese or overweight.
It’s kind of weird that the article doesn’t include this number, which is crucial to contextualising the news.
However, the article does state the following key point:
Just over 42% of the U.S. population was considered obese in 2018, according to the agency’s most recent statistics. Overweight is defined as having a body mass index of 25 or more, while obesity is defined as having a BMI of 30 or more.
…and upon re-reading, I can see that was a poorly presented key point.
Which looks like an astounding stat until you look uo that 73% of American adults are obese or overweight.
It’s kind of weird that the article doesn’t include this number, which is crucial to contextualising the news.
However, the article does state the following key point:
Just over 42% of the U.S. population was considered obese in 2018, according to the agency’s most recent statistics. Overweight is defined as having a body mass index of 25 or more, while obesity is defined as having a BMI of 30 or more.
I know, and that’s terrible. That’s just going to mislead the audience. Why not take five seconds to look up the relevant statistic and include that?
Which looks like an astounding stat until you look uo that 73% of American adults are obese or overweight.
It’s kind of weird that the article doesn’t include this number, which is crucial to contextualising the news.
However, the article does state the following key point:
Just over 42% of the U.S. population was considered obese in 2018, according to the agency’s most recent statistics. Overweight is defined as having a body mass index of 25 or more, while obesity is defined as having a BMI of 30 or more.
I know, and that’s terrible. That’s just going to mislead the audience. Why not take five seconds to look up the relevant statistic and include that?
So… a bloke on another forum heads up an ICU in a major capital city must have gotten on the sauce last night and posted this:
Oh we are seriously fucked.
Many signs the system is already heaving.
It is currently taking us about 24 hours to get a swab result back. We only have 36 rapid swabs to last us 3 months – we are literally slap bang in the middle of COVID central.
We had a death right at the start of the week. This has gone unreported in all the pressers. Family at that stage had refused to be tested and not following quarantining requirements. We know through other means that DHHS has not followed up. They’re out there living their best lives almost certainly spreading it.
Most telling was the DCHO refusing to answer a question when interviewed by the ABC last night about whether the contact tracing was overwhelmed.
It is clear Old Mate was counting on a zero covid strategy because we seem completely unprepared for what looks to be a much worse wave than last year.
‘Queensland records no new COVID-19 cases
Queensland records zero new cases of COVID-19, Premier Annastacia Palaszczuk announces.’
Scomo and SadGlad keep telling Anastacia that the Qld measures just won’t work, but, in rude and inconsiderate defiance of that, they do.
Oh, the arrival of and spread of Delta in Qld is inevitable, no arguments.
But i think that what the Qld govt is trying to do is just buy as much time as they can. For Qld to get its immunised numbers up, for NSW and Vic to get their immunised numbers up, maybe for the wave to peak and begin to decline and the number of carriers and spreaders in and from those States to also begin to decline, all with the aim of minimising the impact on Qld.
Just because someone tells you that you can’t save your house from the bushfire doesn’t mean that you should drop the hose and run into the middle of it.
And further…when I’m driving sometimes my mind wanders (when NewsRadio goes to sport, for instance). So…Sweden again. Because as an experiment, they are interesting. With the soft measures last year because of their Constitution, and I don’t think they closed primary schools, would this mean that their younger folk possibly/probably developed levels of immunity by running low to no symptom infections through that part of the population? They have fairly high vaccination levels now too:
Sweden
Doses given 12.7M
Fully vaccinated 5.79M
% of population fully vaccinated 56.6%
(Ref: ourworldindata)
So all in all, there should be quite high levels of immunity in the Swedish population by now.
NSW breaks COVID-19 infection records with 1,431 new cases and 12 deaths
yay for them!
One of those deaths was a woman who died at home the day after she tested positive. It was mentioned she was unvaccinated, but being in her 30s, she’d apparently only been eligable for vaccinated for a week.
NSW breaks COVID-19 infection records with 1,431 new cases and 12 deaths
Bjelkean is saying that next week will see the peak.
If she can foretell the future like that, why the hell hasn’t she been telling us in advance before?
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
Bjelkean is saying that next week will see the peak.
If she can foretell the future like that, why the hell hasn’t she been telling us in advance before?
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
Dan had to do that. For weeks and weeks and weeks. Then he slipped down some stairs and had some months off…now he gets to do it all over again.
‘Queensland records no new COVID-19 cases
Queensland records zero new cases of COVID-19, Premier Annastacia Palaszczuk announces.’
Scomo and SadGlad keep telling Anastacia that the Qld measures just won’t work, but, in rude and inconsiderate defiance of that, they do.
Oh, the arrival of and spread of Delta in Qld is inevitable, no arguments.
But i think that what the Qld govt is trying to do is just buy as much time as they can. For Qld to get its immunised numbers up, for NSW and Vic to get their immunised numbers up, maybe for the wave to peak and begin to decline and the number of carriers and spreaders in and from those States to also begin to decline, all with the aim of minimising the impact on Qld.
Just because someone tells you that you can’t save your house from the bushfire doesn’t mean that you should drop the hose and run into the middle of it.
the language and notion of inevitability is like a black hole, a conceptual implosion device delivered to psychological primitives so that they might be inclined to share the beauty of it, and it very successfully vanishes the working imaginations of those it inhabits, leaves them with no soul, even inspires terrorism to make certain the inevitable is really inevitable
has a recursion about it, a non-specificity of what it will likely be applied, it floats around looking for things to settle in, to do its good work
Bjelkean is saying that next week will see the peak.
If she can foretell the future like that, why the hell hasn’t she been telling us in advance before?
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
…and then going home at night knowing your playing politics has directly caused dozens of deaths.
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
She listened to the health experts, but acted on what the business lobbyists and Liberal party wise guys told her.
She made her bed, and she can damn well lie in in it.
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
She listened to the health experts, but acted on what the business lobbyists and Liberal party wise guys told her.
She made her bed, and she can damn well lie in in it.
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
She listened to the health experts, but acted on what the business lobbyists and Liberal party wise guys told her.
She made her bed, and she can damn well lie in in it.
I am just so effing angry with Gladys.
This will be her legacy – the Premier who fucked it all up.
Doherty Inst model suggests that opening at 70-80% will result in 2000 to 3000 deaths per year. ie about 38 to 58 deaths per week nationwide. If NSW had a proportional share, that’s about 13 to 19 deaths per week in NSW.
Currently NSW is at 40% ie there are about a two thirds reduction in the numbar of not fully vaxed people as they move to 80%. NSW has incurred 38 deaths in the last week. If we assume the “opportunity to die “ also decreases by 2/3 then I suppose that means about 13 deaths a week which is right in line with the DohInsMod… except that the NSW is already on lockdown.
So I’m hoping that the plan is just to blast through 80% and try to get to 98 or 99% or something.
‘Queensland records no new COVID-19 cases
Queensland records zero new cases of COVID-19, Premier Annastacia Palaszczuk announces.’
Scomo and SadGlad keep telling Anastacia that the Qld measures just won’t work, but, in rude and inconsiderate defiance of that, they do.
Oh, the arrival of and spread of Delta in Qld is inevitable, no arguments.
But i think that what the Qld govt is trying to do is just buy as much time as they can. For Qld to get its immunised numbers up, for NSW and Vic to get their immunised numbers up, maybe for the wave to peak and begin to decline and the number of carriers and spreaders in and from those States to also begin to decline, all with the aim of minimising the impact on Qld.
Just because someone tells you that you can’t save your house from the bushfire doesn’t mean that you should drop the hose and run into the middle of it.
the language and notion of inevitability is like a black hole, a conceptual implosion device delivered to psychological primitives so that they might be inclined to share the beauty of it, and it very successfully vanishes the working imaginations of those it inhabits, leaves them with no soul, even inspires terrorism to make certain the inevitable is really inevitable
has a recursion about it, a non-specificity of what it will likely be applied, it floats around looking for things to settle in, to do its good work
Imagine doctors working for better health and saving lives.
When asked what level of death she would be comfortable with, Dr Young replied: “I’m a doctor, none.” “Come on, can you please remember who I am? I stand up here every day but ultimately, I went into medicine to save lives, I’m not comfortable with any deaths that are preventable,” she said.
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
She listened to the health experts, but acted on what the business lobbyists and Liberal party wise guys told her.
She made her bed, and she can damn well lie in in it.
Yes.
Strange thing is though, that overall the economy is not quite so hard hit by the lockdowns and travel restrictions as much as some people were expecting. It has not been an economic disaster. So the case against locking down is not quite so strong.
Doherty Inst model suggests that opening at 70-80% will result in 2000 to 3000 deaths per year. ie about 38 to 58 deaths per week nationwide. If NSW had a proportional share, that’s about 13 to 19 deaths per week in NSW.
Currently NSW is at 40% ie there are about a two thirds reduction in the numbar of not fully vaxed people as they move to 80%. NSW has incurred 38 deaths in the last week. If we assume the “opportunity to die “ also decreases by 2/3 then I suppose that means about 13 deaths a week which is right in line with the DohInsMod… except that the NSW is already on lockdown.
So I’m hoping that the plan is just to blast through 80% and try to get to 98 or 99% or something.
Also already being on lockdown aside, is that model for when starting from a near-zero-COVID number of cases ¿
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
She listened to the health experts, but acted on what the business lobbyists and Liberal party wise guys told her.
She made her bed, and she can damn well lie in in it.
Yes.
Strange thing is though, that overall the economy is not quite so hard hit by the lockdowns and travel restrictions as much as some people were expecting. It has not been an economic disaster. So the case against locking down is not quite so strong.
Well yes because travel from external sources is generally like only 10% of economic turnover. Yet bizarrely the alarmist case against lockdown seems as loud if not louder than ever.
I don’t think the government should be setting targets like 70% or 80% before lifting restrictions. I think it should be a case of everyone that wants to be vaccinated has had their two doses. When that happens we can lift restrictions, and teh remaining voluntarily unvaccinated can take their chances.
But Gutless Binchicken is happily appeasing both sides by not actually making any big reopening moves while telling everyone that the reopening moves are happening as we speak.
I don’t think the government should be setting targets like 70% or 80% before lifting restrictions. I think it should be a case of everyone that wants to be vaccinated has had their two doses. When that happens we can lift restrictions, and teh remaining voluntarily unvaccinated can take their chances.
What about senile or juvenile people who don’t know what it means to want to be vaccinated¿
I don’t think the government should be setting targets like 70% or 80% before lifting restrictions. I think it should be a case of everyone that wants to be vaccinated has had their two doses. When that happens we can lift restrictions, and teh remaining voluntarily unvaccinated can take their chances.
And no vaccination card will get you to the back of the line for triage or a ventilator.
I don’t think the government should be setting targets like 70% or 80% before lifting restrictions. I think it should be a case of everyone that wants to be vaccinated has had their two doses. When that happens we can lift restrictions, and teh remaining voluntarily unvaccinated can take their chances.
What about senile or juvenile people who don’t know what it means to want to be vaccinated¿
They have a guardian or parent that can make that decision for them.
I don’t think the government should be setting targets like 70% or 80% before lifting restrictions. I think it should be a case of everyone that wants to be vaccinated has had their two doses. When that happens we can lift restrictions, and teh remaining voluntarily unvaccinated can take their chances.
What about senile or juvenile people who don’t know what it means to want to be vaccinated¿
And those people who want the other brand that will be here soon and has been will be here soon for the past 8 months ¿
I don’t think the government should be setting targets like 70% or 80% before lifting restrictions. I think it should be a case of everyone that wants to be vaccinated has had their two doses. When that happens we can lift restrictions, and teh remaining voluntarily unvaccinated can take their chances.
And no vaccination card will get you to the back of the line for triage or a ventilator.
So do we agree it’s reasonable to wait until approval and delivery of vaccines for ages down to 2 years ¿
I don’t think the government should be setting targets like 70% or 80% before lifting restrictions. I think it should be a case of everyone that wants to be vaccinated has had their two doses. When that happens we can lift restrictions, and teh remaining voluntarily unvaccinated can take their chances.
I don’t think the government should be setting targets like 70% or 80% before lifting restrictions. I think it should be a case of everyone that wants to be vaccinated has had their two doses. When that happens we can lift restrictions, and teh remaining voluntarily unvaccinated can take their chances.
What about senile or juvenile people who don’t know what it means to want to be vaccinated¿
And those people who want the other brand that will be here soon and has been will be here soon for the past 8 months ¿
I can’t remember ever being aware of the brand of my vaccination before this. You get whatever fluvax is going. Same with tetanus etc etc.
“South Australian health authorities say they are stunned a person booked a COVID-19 vaccination appointment 40 times, blocking dozens of other people from receiving a dose.
It comes as regional health officials renew calls for people to turn up to vaccine appointments following a string of people not attending their allocated booking time.”
What about senile or juvenile people who don’t know what it means to want to be vaccinated¿
And those people who want the other brand that will be here soon and has been will be here soon for the past 8 months ¿
I can’t remember ever being aware of the brand of my vaccination before this. You get whatever fluvax is going. Same with tetanus etc etc.
Hey we’re not suggesting it’s right to compare (though unlike many other medical products, it is not the case that the active ingredients are very similar), we’re specifically asking whether it’s acceptable to hold off threatening unvaccinated people with exposure, if they’re still waiting for access to a brand of product that was claim-offered long ago but not deliver-offered as yet.
“South Australian health authorities say they are stunned a person booked a COVID-19 vaccination appointment 40 times, blocking dozens of other people from receiving a dose.
It comes as regional health officials renew calls for people to turn up to vaccine appointments following a string of people not attending their allocated booking time.”
“South Australian health authorities say they are stunned a person booked a COVID-19 vaccination appointment 40 times, blocking dozens of other people from receiving a dose.
It comes as regional health officials renew calls for people to turn up to vaccine appointments following a string of people not attending their allocated booking time.”
I think there is an element of wishful thinking in that. Must be a tough gig fronting up each day to announce a new record number of cases, beating the mark set the previous day.
She listened to the health experts, but acted on what the business lobbyists and Liberal party wise guys told her.
She made her bed, and she can damn well lie in in it.
I am just so effing angry with Gladys.
you can be sure it’s costing much much more than staying with a committed elimination objective, and way more inconvenient, this will all continue way beyond christmas, way way beyond, mainly because of the deceptions employed is my personal view
the rot started with a plan to release a biological hazard back to nature, and calling it opening up
The Bin-chicken hasn’t told us how many people are in ICU, nor the numbers on ventilators. And she talks “But we’re also going through both the exciting but challenging time of opening up.”
“South Australian health authorities say they are stunned a person booked a COVID-19 vaccination appointment 40 times, blocking dozens of other people from receiving a dose.
It comes as regional health officials renew calls for people to turn up to vaccine appointments following a string of people not attending their allocated booking time.”
I am expressing exasperation at, and lack of understanding of, some people’s actions.
Pretty sure a while back there were posts about antivaccination groups planning exactly this tactic of booking and blocking appointments simply to further their own agenda. We understand that. We think it’s fucked up, but we understand how they reach that fucked upedness.
I am expressing exasperation at, and lack of understanding of, some people’s actions.
Pretty sure a while back there were posts about antivaccination groups planning exactly this tactic of booking and blocking appointments simply to further their own agenda. We understand that. We think it’s fucked up, but we understand how they reach that fucked upedness.
I don’t understand how they reach their conclusions.
you can be sure it’s costing much much more than staying with a committed elimination objective, and way more inconvenient, this will all continue way beyond christmas, way way beyond, mainly because of the deceptions employed is my personal view
the rot started with a plan to release a biological hazard back to nature, and calling it opening up
The Bin-chicken hasn’t told us how many people are in ICU, nor the numbers on ventilators. And she talks “But we’re also going through both the exciting but challenging time of opening up.”
It’ll cost less, because all they do is reduce the care provided for other things, and like magic, hospitals have spare capacity, they’re not overwhelmed, we don’t have to pay for the other things. Then people die of other things (not COVID-19) so it’s not a pandemic problem, but it’s all right, because they were old / useless / conditionally preexisting / going to die anyway, and cost the health system less too. Magic¡
About ICU and ventilators, word from people we know in NSW is that they’ve actually had to expand ICUs into adjacent wards. Make of that what you will.
I am expressing exasperation at, and lack of understanding of, some people’s actions.
Pretty sure a while back there were posts about antivaccination groups planning exactly this tactic of booking and blocking appointments simply to further their own agenda. We understand that. We think it’s fucked up, but we understand how they reach that fucked upedness.
I don’t understand how they reach their conclusions.
Fair. If we survive this pandemic then our SCIENCE classes are going to fundamentally shift to a predominance of critical thinking education. Not that our students are bad at it compared to others as far as we see, but we need everyone to be so much better.
Pretty sure a while back there were posts about antivaccination groups planning exactly this tactic of booking and blocking appointments simply to further their own agenda. We understand that. We think it’s fucked up, but we understand how they reach that fucked upedness.
I don’t understand how they reach their conclusions.
Fair. If we survive this pandemic then our SCIENCE classes are going to fundamentally shift to a predominance of critical thinking education. Not that our students are bad at it compared to others as far as we see, but we need everyone to be so much better.
PM announces a 4 million dose vaccine swap deal with the United Kingdom
Australia will receive 4 million doses of the Pfizer vaccine months earlier than expected after a major vaccine swap deal with the UK.
The British doses will arrive in Australia this month to allow them to be used before they expire.
Australia will return the favour later in the year by sending 4 million of its future stockpile back to the UK.
The doses will be distributed across Australia based on the population of each state and territory.
Isn’t that a bit unfair; shouldn’t NSW be getting all of them?
PM announces a 4 million dose vaccine swap deal with the United Kingdom
Australia will receive 4 million doses of the Pfizer vaccine months earlier than expected after a major vaccine swap deal with the UK.
The British doses will arrive in Australia this month to allow them to be used before they expire.
Australia will return the favour later in the year by sending 4 million of its future stockpile back to the UK.
The doses will be distributed across Australia based on the population of each state and territory.
Isn’t that a bit unfair; shouldn’t NSW be getting all of them?
Gladys should be getting them to hand out personally to friends and relatives.
PM announces a 4 million dose vaccine swap deal with the United Kingdom
Australia will receive 4 million doses of the Pfizer vaccine months earlier than expected after a major vaccine swap deal with the UK.
The British doses will arrive in Australia this month to allow them to be used before they expire.
Australia will return the favour later in the year by sending 4 million of its future stockpile back to the UK.
The doses will be distributed across Australia based on the population of each state and territory.
Isn’t that a bit unfair; shouldn’t NSW be getting all of them?
Gladys should be getting them to hand out personally to friends and relatives.
Tasmania has a greater % of oldies so perhaps they should get extra
PM announces a 4 million dose vaccine swap deal with the United Kingdom
Australia will receive 4 million doses of the Pfizer vaccine months earlier than expected after a major vaccine swap deal with the UK.
The British doses will arrive in Australia this month to allow them to be used before they expire.
Australia will return the favour later in the year by sending 4 million of its future stockpile back to the UK.
The doses will be distributed across Australia based on the population of each state and territory.
Isn’t that a bit unfair; shouldn’t NSW be getting all of them?
Gladys should be getting them to hand out personally to friends and relatives.
Tasmania has a greater % of oldies so perhaps they should get extra
We also have lots of disability pensioners. I know a bunch that purposefully moved to Tasmania because even though the medical system might not be as good as some other states when they moved here it was cheap to get housing. (that is no longer the case)
But Tassie folk seem to be taking vaccination more seriously than some other states.
you can be sure it’s costing much much more than staying with a committed elimination objective, and way more inconvenient, this will all continue way beyond christmas, way way beyond, mainly because of the deceptions employed is my personal view
the rot started with a plan to release a biological hazard back to nature, and calling it opening up
The Bin-chicken hasn’t told us how many people are in ICU, nor the numbers on ventilators. And she talks “But we’re also going through both the exciting but challenging time of opening up.”
It’ll cost less, because all they do is reduce the care provided for other things, and like magic, hospitals have spare capacity, they’re not overwhelmed, we don’t have to pay for the other things. Then people die of other things (not COVID-19) so it’s not a pandemic problem, but it’s all right, because they were old / useless / conditionally preexisting / going to die anyway, and cost the health system less too. Magic¡
About ICU and ventilators, word from people we know in NSW is that they’ve actually had to expand ICUs into adjacent wards. Make of that what you will.
it’s costing a shitload more than maintaining the elimination objective, or vaccine+ if you will
it’s going to be protracted, nasty, full of bullshit, endless deceptions
there are a few politicians probably opening up a new tube of slippery while watching the escape of the contagion, some media also, and others, a lot of low-level psychopaths recruited and recruiting for covid egalitarianism
The Bin-chicken hasn’t told us how many people are in ICU, nor the numbers on ventilators. And she talks “But we’re also going through both the exciting but challenging time of opening up.”
It’ll cost less, because all they do is reduce the care provided for other things, and like magic, hospitals have spare capacity, they’re not overwhelmed, we don’t have to pay for the other things. Then people die of other things (not COVID-19) so it’s not a pandemic problem, but it’s all right, because they were old / useless / conditionally preexisting / going to die anyway, and cost the health system less too. Magic¡
About ICU and ventilators, word from people we know in NSW is that they’ve actually had to expand ICUs into adjacent wards. Make of that what you will.
it’s costing a shitload more than maintaining the elimination objective, or vaccine+ if you will
it’s going to be protracted, nasty, full of bullshit, endless deceptions
there are a few politicians probably opening up a new tube of slippery while watching the escape of the contagion, some media also, and others, a lot of low-level psychopaths recruited and recruiting for covid egalitarianism
Clear enough to our minds. Aim for zero, elimination, and your upfront costs are
subsidy for waiting to workers
build decent healthcare / quarantine facilities, only required once no matter how many times you aim to eliminate
until you get there, and then your ongoing costs are
quarantine
usual healthcare costs for a privileged, demanding population that wants healthcare provided at the level of quality that they’re used to
but Let It Rip™, Throw It All Open, Dive Into The Cesspool and your upfront costs are
NOTHING¡ WIN¡
while your ongoing costs are
acutely unwell workers
chronically unwell workers
dead workers
fearful refusing to workers
the same healthcare costs as before but now directed to an entirely preventable disease
. We mean, the choice is obvious, only one of those has an upfront cost so the other one is undeniably better.
It’ll cost less, because all they do is reduce the care provided for other things, and like magic, hospitals have spare capacity, they’re not overwhelmed, we don’t have to pay for the other things. Then people die of other things (not COVID-19) so it’s not a pandemic problem, but it’s all right, because they were old / useless / conditionally preexisting / going to die anyway, and cost the health system less too. Magic¡
About ICU and ventilators, word from people we know in NSW is that they’ve actually had to expand ICUs into adjacent wards. Make of that what you will.
it’s costing a shitload more than maintaining the elimination objective, or vaccine+ if you will
it’s going to be protracted, nasty, full of bullshit, endless deceptions
there are a few politicians probably opening up a new tube of slippery while watching the escape of the contagion, some media also, and others, a lot of low-level psychopaths recruited and recruiting for covid egalitarianism
Clear enough to our minds. Aim for zero, elimination, and your upfront costs are
subsidy for waiting to workers
build decent healthcare / quarantine facilities, only required once no matter how many times you aim to eliminate
until you get there, and then your ongoing costs are
quarantine
usual healthcare costs for a privileged, demanding population that wants healthcare provided at the level of quality that they’re used to
but Let It Rip™, Throw It All Open, Dive Into The Cesspool and your upfront costs are
NOTHING¡ WIN¡
while your ongoing costs are
acutely unwell workers
chronically unwell workers
dead workers
fearful refusing to workers
the same healthcare costs as before but now directed to an entirely preventable disease
. We mean, the choice is obvious, only one of those has an upfront cost so the other one is undeniably better.
Queensland has confirmed one new case of COVID-19, a four-year-old girl who is a close contact of a Logan truck driver who tested positive to the Delta strain of the virus earlier this week.
Authorities say the child attended the Boulevard Early Learning Centre at Mount Warren Park, on the outskirts of Logan, south of Brisbane, on Tuesday and Wednesday.
Children, staff and visitors to the centre have been asked to immediately come forward for testing and then quarantine at home for 14 days, even if they get a negative result.
The early learning centre is also used for after-school care for children at Windaroo State School in Logan.
Students, staff and visitors who’ve been at Windaroo State School from Tuesday to Friday, and all their household members, now need to quarantine for 14 days.
More to come.
—
and we thought the authorities said that children don’t spread disease
In Australia, it hasn’t peaked but the rate of growth has shrunk a bit.
So, this peak in Australia should be over within two months.
The mortality rate from Australia’s delta wave is much less than I had been led to believe by OurWorldInData. Because of the imposition of smoothing and ignoring the time delay in OurWorldInData. We’re back close to our original 0.7% mortality, the same as the first wave.
It may ber worth my doing a data analysis on the delta wave myself.
Queensland has confirmed one new case of COVID-19, a four-year-old girl who is a close contact of a Logan truck driver who tested positive to the Delta strain of the virus earlier this week.
Authorities say the child attended the Boulevard Early Learning Centre at Mount Warren Park, on the outskirts of Logan, south of Brisbane, on Tuesday and Wednesday.
Children, staff and visitors to the centre have been asked to immediately come forward for testing and then quarantine at home for 14 days, even if they get a negative result.
The early learning centre is also used for after-school care for children at Windaroo State School in Logan.
Students, staff and visitors who’ve been at Windaroo State School from Tuesday to Friday, and all their household members, now need to quarantine for 14 days.
More to come.
—
and we thought the authorities said that children don’t spread disease
fuck all the psychopaths
Bloody Bin-chicken exporting disease by not doing what was agreed: hard and fast.
Queensland has confirmed one new case of COVID-19, a four-year-old girl who is a close contact of a Logan truck driver who tested positive to the Delta strain of the virus earlier this week.
Authorities say the child attended the Boulevard Early Learning Centre at Mount Warren Park, on the outskirts of Logan, south of Brisbane, on Tuesday and Wednesday.
Children, staff and visitors to the centre have been asked to immediately come forward for testing and then quarantine at home for 14 days, even if they get a negative result.
The early learning centre is also used for after-school care for children at Windaroo State School in Logan.
Students, staff and visitors who’ve been at Windaroo State School from Tuesday to Friday, and all their household members, now need to quarantine for 14 days.
More to come.
—
and we thought the authorities said that children don’t spread disease
fuck all the psychopaths
There is no evidence in that report that the child has spread the disease.
Queensland has confirmed one new case of COVID-19, a four-year-old girl who is a close contact of a Logan truck driver who tested positive to the Delta strain of the virus earlier this week.
Authorities say the child attended the Boulevard Early Learning Centre at Mount Warren Park, on the outskirts of Logan, south of Brisbane, on Tuesday and Wednesday.
Children, staff and visitors to the centre have been asked to immediately come forward for testing and then quarantine at home for 14 days, even if they get a negative result.
The early learning centre is also used for after-school care for children at Windaroo State School in Logan.
Students, staff and visitors who’ve been at Windaroo State School from Tuesday to Friday, and all their household members, now need to quarantine for 14 days.
More to come.
—
and we thought the authorities said that children don’t spread disease
fuck all the psychopaths
There is no evidence in that report that the child has spread the disease.
there is evidence that they’re worried about it so maybe they’re lying then
Queensland has confirmed one new case of COVID-19, a four-year-old girl who is a close contact of a Logan truck driver who tested positive to the Delta strain of the virus earlier this week.
Authorities say the child attended the Boulevard Early Learning Centre at Mount Warren Park, on the outskirts of Logan, south of Brisbane, on Tuesday and Wednesday.
Children, staff and visitors to the centre have been asked to immediately come forward for testing and then quarantine at home for 14 days, even if they get a negative result.
The early learning centre is also used for after-school care for children at Windaroo State School in Logan.
Students, staff and visitors who’ve been at Windaroo State School from Tuesday to Friday, and all their household members, now need to quarantine for 14 days.
More to come.
—
and we thought the authorities said that children don’t spread disease
fuck all the psychopaths
There is no evidence in that report that the child has spread the disease.
there is evidence that they’re worried about it so maybe they’re lying then
It could be that the increased viral loads of delta mean that what was once negligible transmission is now an issue.
I wonder whether Covid is having a positive effect of encouraging people to get more exercise, in that people who previously did zero exercise as now doing non-zero exercise as that’s a valid reason to be out of the house.
I am expressing exasperation at, and lack of understanding of, some people’s actions.
Pretty sure a while back there were posts about antivaccination groups planning exactly this tactic of booking and blocking appointments simply to further their own agenda. We understand that. We think it’s fucked up, but we understand how they reach that fucked upedness.
I don’t understand how they reach their conclusions.
Just encountered this, perhaps a start but probably doesn’t explain the crazy ones.
The delta variant is not just the dominant strain in the world today, it’s more prevalent than that.
In more than 90% of countries that report variants, more than 97% of cases are delta variant.
Keeping in mind that the delta variant is new. There is hardly any country in the world that pays even lip suervice to border quarantine
27/07/2021 looks to be a critical date for the Delta strain. For more than 50% of countries that are now dominated by the Delta strain, they reported fewer than 40% Delta strain before that date and 80% or more Delta strain on and after that date.
Fingers crossed, that should make calculating the mortality rate (as opposed to the case fatality rate which is a less accurate calculation) for the Delta strain in eighty or so countries really easy.
I’m doing this to see whether the Delta strain has a single mortality rate or a mortality rate that varies from country to country in a systematic way.
The delta variant is not just the dominant strain in the world today, it’s more prevalent than that.
In more than 90% of countries that report variants, more than 97% of cases are delta variant.
Keeping in mind that the delta variant is new. There is hardly any country in the world that pays even lip suervice to border quarantine
27/07/2021 looks to be a critical date for the Delta strain. For more than 50% of countries that are now dominated by the Delta strain, they reported fewer than 40% Delta strain before that date and 80% or more Delta strain on and after that date.
Fingers crossed, that should make calculating the mortality rate (as opposed to the case fatality rate which is a less accurate calculation) for the Delta strain in eighty or so countries really easy.
I’m doing this to see whether the Delta strain has a single mortality rate or a mortality rate that varies from country to country in a systematic way.
So do you think it has much further to go in evolution or is it starting to reach the limit of biophysichemistry¿
The delta variant is not just the dominant strain in the world today, it’s more prevalent than that.
In more than 90% of countries that report variants, more than 97% of cases are delta variant.
Keeping in mind that the delta variant is new. There is hardly any country in the world that pays even lip suervice to border quarantine
27/07/2021 looks to be a critical date for the Delta strain. For more than 50% of countries that are now dominated by the Delta strain, they reported fewer than 40% Delta strain before that date and 80% or more Delta strain on and after that date.
Fingers crossed, that should make calculating the mortality rate (as opposed to the case fatality rate which is a less accurate calculation) for the Delta strain in eighty or so countries really easy.
I’m doing this to see whether the Delta strain has a single mortality rate or a mortality rate that varies from country to country in a systematic way.
you might want to dig around re Zn serum levels of different populations, evaluate something of susceptibility to serious illness and death, and also of individuals, check out any possible correlations below and above ~ .50 mcg/mL, could turn up something interesting
In comparison to standard polymerase chain reaction (PCR) tests, the nasal swabbing process for rapid antigen testing is quicker and less invasive. They’re also considerably less expensive. The downside, however, is rapid antigen testing is less accurate than PCR testing – but it’s a comparison Professor Wood says receives undue focus. “That’s actually not the question. The question is, in what circumstances would you use them? “These tests are to complement what we do, not to replace [PCR testing].
Professor Williamson says rapid antigen testing would be particularly useful in workplaces such as health care, aged care, food distribution plants and even construction sites, where people work together in “relatively close quarters.” “The evidence suggests that these tests have the most promising role in frequent testing of the same cohort of people, and that frequent testing can help offset the decrease in sensitivity with the test,” she said.
All right¡ Now watch as Corruption Coalition take this idea, then cut funding for PCR and replace it with occasional rapid antigen testing¡ (Wouldn’t happen anywhere else in the world either would it¿)
So today um we have a special message from Florida man to the people of Australia because a couple of the Australians who watch this channel have sent messages
I guess politicians there in Australia want to relax things
When the public health issue started Australia enacted some pretty strict measures very strict i guess and now there are politicians and commentators there suggesting that they adopt more of a u.s style approach
Okay so to figure out if this is a good idea we’re just going to look at the numbers real quick because i think that might uh be a pretty persuasive argument
The population of Australia is about 25 million that’s roughly the population of Florida
Australia has a little bit more here in Florida we have 21 million people and if you’re in Australia and you don’t know Florida is the Australia of the united states okay
Um similar populations we have lost 45 000 people in Florida alone to this y’all just broke a thousand
You have more people if you were to scale your population up to match the entire population of the united states 328 million i think so uh what 13 times y’all would have lost 13 000 people if you were as big as the us
We have lost 640 000
From Florida man to Australia you want to relax things whatever that’s your country do with it as you choose but please do not follow the united states
As lee we don’t have a clue what we’re doing we are handling this very poorly we have people going to the livestock store to get meds
It’s not going well here we are not an example of anything except what not to do
Do not try to model yourselves after us do not look to the united states and say hey they’re doing all right no we are not
The sound bites that may be filtering over there may be painting a very different picture of uh of what’s going on than the reality
Florida the state that i’m in and quite a few others i want to say five or six have lost one out of every 500 people to this
Do not model yourselves after us
What y’all want to do as far as restrictions and stuff like that that’s all up to you but please do not look to the united states for leadership on this we’re we’re not handling it well
Anyway it’s just a thought you all have a good day
Massive study confirms vaccination reduces risk of long COVID
https://newatlas.com/health-wellbeing/vaccination-reduces-risk-long-covid/
A large study led by researchers from King’s College London has found fully vaccinated adults are around 50 percent less likely to suffer from long COVID if they are unfortunate enough to experience a breakthrough SARS-CoV-2 infection.
If we leave a significant proportion of the population unvaccinated, we run the risk of new, more-difficult-to-deal-with variants evolving, I think.
Mind you, vaccination of adults doesn’t guarantee zero infections and zero transmission, either. So we still run that evolutionary risk.
Morning all.
Don’t know if I mentioned it (chemo brain) but the hematologist says I can get the covid jab 2 weeks after this round of treatment ends. I’m booked for my first shot on the 27th.
If we leave a significant proportion of the population unvaccinated, we run the risk of new, more-difficult-to-deal-with variants evolving, I think.
Mind you, vaccination of adults doesn’t guarantee zero infections and zero transmission, either. So we still run that evolutionary risk.
Morning all.
Don’t know if I mentioned it (chemo brain) but the hematologist says I can get the covid jab 2 weeks after this round of treatment ends. I’m booked for my first shot on the 27th.
If we leave a significant proportion of the population unvaccinated, we run the risk of new, more-difficult-to-deal-with variants evolving, I think.
Mind you, vaccination of adults doesn’t guarantee zero infections and zero transmission, either. So we still run that evolutionary risk.
Morning all.
Don’t know if I mentioned it (chemo brain) but the hematologist says I can get the covid jab 2 weeks after this round of treatment ends. I’m booked for my first shot on the 27th.
If we leave a significant proportion of the population unvaccinated, we run the risk of new, more-difficult-to-deal-with variants evolving, I think.
Mind you, vaccination of adults doesn’t guarantee zero infections and zero transmission, either. So we still run that evolutionary risk.
Morning all.
Don’t know if I mentioned it (chemo brain) but the hematologist says I can get the covid jab 2 weeks after this round of treatment ends. I’m booked for my first shot on the 27th.
Excellent, excellent, excellent news!
:)
Mixed feelings. If it upsets the remarkable effectiveness of the chemo I’d be in a worse state than now.
The nurses look at my blood results before each day’s pair of needles & yesterday one said to me “Well, look at you with your perfect blood”
Morning all.
Don’t know if I mentioned it (chemo brain) but the hematologist says I can get the covid jab 2 weeks after this round of treatment ends. I’m booked for my first shot on the 27th.
Excellent, excellent, excellent news!
:)
Mixed feelings. If it upsets the remarkable effectiveness of the chemo I’d be in a worse state than now.
The nurses look at my blood results before each day’s pair of needles & yesterday one said to me “Well, look at you with your perfect blood”
well all right, so why is a 1 in 500 chance of dying from COVID-19 a simple matter of Let It Rip™ For The Economy Must Grow® but a one in a million chance of getting treatable cancer a pretty big deal ¿
dear God some that work for the Stateblaster, appealing to the globalist borderblasters, will be pulling their hair out hearing of, or seeing these positive sentiments about the States, about borders of any sort, they’ll be pacing up and down corridors muttering release the virus, the Delta++++++++ version
If there is one way that Covid has affected me, it is that I am no longer considering that abolishing the states might be a good idea worth pursuing.
That is just an excuse for not having a competent federal government though.
Yeah, but how do we guarantee a competent federal government? Or a competent state government too for that matter. As long as one of them is competent it can offset the impact of the other’s incompetence. If they are both incompetent it is a problem (refer NSW). Checks and balances and all that.
If there is one way that Covid has affected me, it is that I am no longer considering that abolishing the states might be a good idea worth pursuing.
That is just an excuse for not having a competent federal government though.
Yeah, but how do we guarantee a competent federal government? Or a competent state government too for that matter. As long as one of them is competent it can offset the impact of the other’s incompetence. If they are both incompetent it is a problem (refer NSW). Checks and balances and all that.
by improving the education system. educating the masses on critical thinking. giving more teeth to regulators so that we have truth in advertising at time of elections. Better selection processes for political candidates. less lobbying. less political donations. more penalties, that are actually applied, to pollies that break the rules.
If there is one way that Covid has affected me, it is that I am no longer considering that abolishing the states might be a good idea worth pursuing.
That is just an excuse for not having a competent federal government though.
Yeah, but how do we guarantee a competent federal government? Or a competent state government too for that matter. As long as one of them is competent it can offset the impact of the other’s incompetence. If they are both incompetent it is a problem (refer NSW). Checks and balances and all that.
Any democratic system is only as good as the politicians who participate in it.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
That is just an excuse for not having a competent federal government though.
Yeah, but how do we guarantee a competent federal government? Or a competent state government too for that matter. As long as one of them is competent it can offset the impact of the other’s incompetence. If they are both incompetent it is a problem (refer NSW). Checks and balances and all that.
by improving the education system. educating the masses on critical thinking. giving more teeth to regulators so that we have truth in advertising at time of elections. Better selection processes for political candidates. less lobbying. less political donations. more penalties, that are actually applied, to pollies that break the rules.
:-)
we apologise for being insufficiently skilful in our education work to date and resolve to do better
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
He actually does go to the trouble of pointing this out, but near the end of the article.
I reada couple of par before it told me I could read no farther.
from Quotes…
Diplomacy
“I’m enjoying a week’s break in France. They’ve learned to live with Covid here not lurch from one damaging lockdown to another!”
Alexander DownerThe former Foreign minister enjoys a holiday in France. Most of the country has learnt to live with the virus, except for the 126,000 who didn’t and died.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
He actually does go to the trouble of pointing this out, but near the end of the article.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
He actually does go to the trouble of pointing this out, but near the end of the article.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
Mum’s neighbour is still in hospital, in ICUAFAIK. His daughter who is about 10 years old has also been taken to hospital :(
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
He actually does go to the trouble of pointing this out, but near the end of the article.
Rick Morton will tell it how it is, I think.
I still think he was putting it on in the first bit.
The rate of Covid-19 hospitalisations in New South Wales is being reported at one-third of the real figure, with the actual numbers being masked by a decision to only report those who end up in medical facilities, and not the thousands receiving care under the state’s “hospital in the home” arrangements.
On Tuesday, Premier Gladys Berejiklian said the “most recent figure I have for the rate of hospitalisation was 5.5 per cent in terms of cases converting to hospitalisation”. The real figure, however, is about 15 per cent, according to medical experts and a briefing provided to national cabinet.
On Thursday, the state reported almost 1000 people with Covid-19 were in hospital and 160 of those were receiving the most complex form of healthcare in intensive care units.
But that figure leaves out almost 1700 people who are receiving hospital-grade care for coronavirus in their own homes in NSW. Most of those are being monitored by staff from the swamped Westmead Hospital in the state’s Western Sydney Local Health District. Under these arrangements, patients who would otherwise be on the hospital ward are instead given oxygen and other support at home with scheduled visits from hospital staff.
At least eight people in the state have died at home since the Delta outbreak began. Some, who were being given home care, deteriorated so quickly from mild illness to death that there was no time for even an ambulance to be called. The coroner is investigating these deaths.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
The CHRIS platform, developed last year in response to Covid-19, is the same platform used to prepare briefings for national cabinet. In just three weeks the number of staffed ICU beds in NSW has actually fallen by nine.
In advice prepared for national cabinet, hospital demand in all states and territories was forecast using a “transition ratio” from active Covid-19 case to hospitalisation. In the document, obtained by The Saturday Paper, political leaders were told this ratio was calculated by dividing the number of individuals requiring hospitalisation by the number of active cases in the week before. By this method, the hospitalisation ratio is 0.16 or 16 per cent.
Garvan Institute of Medical Research executive director Professor Christopher Goodnow told staff in a private briefing that “hospitalisation is tracking around 15 per cent in the current NSW outbreak”.
These figures are important because health system workers who have spoken with The Saturday Paper believe clinical care is already being compromised in the NSW outbreak and may have already caused the death of people who might otherwise have been saved.
Australian and New Zealand Intensive Care Society president Dr Anthony Holley, whose organisation is advising national cabinet, is blunt.
“The imposition of Covid on the system and the challenge and the stress that is in place cannot and should not be underestimated,” he told The Saturday Paper. “There will be implications. I am deeply concerned and would never underestimate the situation, but I am also confident the professionalism of the front-line workers is such that they will minimise those implications.”
Intensive care paramedic and delegate for the NSW branch of the Australian Paramedics Association Brett Simpson says the ambulance service in the state has already moved beyond its capacity to cope.
Last year, about 170 nursing and healthcare staff were trained to help expand the ICU… only five have expressed an interest in returning.
“You can increase ICU capacity all you want but if we can’t get you to the hospital alive then what’s the point? The ambulance service is not coping in any sense of the word. What we are seeing at the moment are outrageous response times,” he says.
“The worst example I was given last week is a crew from Bateau Bay on the Central Coast having to run lights and sirens to South Granville in Sydney for a house of people with Covid who were all short of breath. Ordinarily, that is a 1.5-hour drive. The distance is 100 kilometres. It is far from an isolated incident. Crews are having to drive half an hour to reach a patient in cardiac arrest,” Simpson said.
Time and again healthcare workers have made the point to this newspaper that it is not just Covid-19 patients who are affected by the system pressure. Everyone who needs medical attention is at risk.
In Liverpool, in the South Western Sydney Local Health District, a 50-year-old man fell three metres from the roof of his house and suffered severe leg injuries, including a horrific “degloving” of his lower left leg.
“After half an hour, when the ambulance just simply hadn’t turned up, his wife dragged him to the car and drove him to Liverpool Hospital on her own – and this is happening more and more and more often,” Simpson says. “The entire health system, despite whatever is happening with Covid and bed block , people are still having heart attacks, they are still having strokes, car and truck accidents, industrial accidents.
“At the moment we are seeing hot jobs sitting in the queue waiting over an hour for an ambulance even to be dispatched on it, let alone get a paramedic crew arriving on the scene.”
By Simpson’s telling, the hospital emergency department network is so finely calibrated that when one becomes overwhelmed, the spillover affects another and another. They fall like dominoes.
The Saturday Paper has obtained a new “patient allocation matrix” for emergency admissions in NSW hospitals that dictates what facilities are available for certain categories of illness. On August 25, the document was circulated to paramedics with two new categories: confirmed Covid-19 and suspected Covid-19.
Of the 46 hospitals – mostly public, with some private – in the local health districts covering the Newcastle–Hunter region, the Central Coast, all of Greater Sydney and Wollongong–Shoalhaven, fewer than half, or 19, are accepting confirmed Covid-19 patients.
In the Western Sydney Local Health District, only Westmead is listed as accepting confirmed cases. Auburn, Blacktown and Mount Druitt will not. Similarly, in the Nepean Blue Mountains Local Health District, only Nepean Hospital is taking admissions for the infection. In south-western Sydney, Liverpool and Campbelltown hospitals are taking Covid-19 patients but Bankstown, Fairfield and Bowral are not.
The only health district so far open for all Covid-19 confirmed and suspected cases is the Northern Sydney region. On Tuesday night, ambulance cars trying to get patients into Westmead, but facing severe bed block, were told to go to the Northern Beaches Hospital almost 35 kilometres away.
As hospitals fill, the domino-effect described by Simpson will become more pronounced.
Another person familiar with the situation among paramedics, who asked not to be named, told The Saturday Paper the bed block, or ramping, of vehicles at Sydney hospitals is now so bad that hospital healthcare workers are X-raying patients in the back of ambulances and providing some early treatment before patients can be sorted into those cases urgent enough to warrant entry.
In the final week of August, major hospitals across the network erected tents at their entrances to help triage Covid-19 patients. But their use differs between each facility. At Royal Prince Alfred Hospital in Camperdown, for example, the mini field hospital has spaced seating for about six patients with Covid-19 to be assessed and treated while waiting for admission. At Westmead, one of the largest hospitals in Australia, the Covid tents are being used to assess patients and offer very basic initial treatment, such as fluids or a Covid-19 test, before sending them back into the ambulances in which they came.
A senior health official said there was a delay in erecting the tents because authorities were worried it would be a “bad look” if the public saw hospital staff in full protective equipment treating people in makeshift marquees. This reluctance made the ambulance bed block issue even worse.
Last weekend, 17 ambulances were bed blocked at Westmead Hospital. As another source says: “That has never happened at any time in the history of the state.”
On Wednesday, Gladys Berejiklian told reporters that “the worst hospitalisation rate is likely to be in October”.
She said: “The most recent advice that I have received is that case numbers are likely to continue to rise in the next few weeks. We know that there is always a lag between when someone gets ill and when they end up in hospital and we anticipate that given where the case numbers are, and given the rate of vaccination, that the highest rate of hospitalisation will occur at some stage in October.”
Nursing staff and doctors are worried about what happens between now and then. The health network is already fragile and so finely calibrated that the pressure threatens to cascade without some intervention.
A source familiar with the operation of Lismore Base Hospital in the state’s northern rivers district says the facility, which has been designated the Covid-19 hospital for the Northern NSW Local Health District, has just four ICU beds. Currently, all of these are occupied by patients without Covid-19.
“As it stands, there are only 4.5 full-time ICU nurses to cover 24/7 care, less than half of the staffing that is needed to cover the weekly roster,” the source says. “Two ICU supervising doctors out of four have been redeployed to Sydney and there is currently no formal agreement between NSW and Queensland regarding what happens to all the northern NSW residents that rely on medical care across the border.
“It is a total shitshow. Paramedics, nurses and other operational staff cannot cross the border with ease at the moment and all key services are having major staffing issues.”
Where once a health crisis in one part of Australia could be met with support from other jurisdictions, the Delta variant represents a risk that has never before been seen.
On Wednesday, Victorian Premier Daniel Andrews announced a dramatic shift in the state’s thinking about Covid-19. The Delta variant outbreak that was seeded from NSW can no longer be controlled, he said.
“We have thrown everything at it, but it is now clear to us that we are not going to drive these numbers down, they’re instead going to increase,” he conceded at a press conference.
Behind the scenes, the situation is more severe than even that update allowed. Data from the Critical Health Resource Information System shows that 391 of the 429 currently staffed ICU beds in Victoria – 91 per cent – are occupied. Of these, 20 are being used for Covid-19 patients – but that number is expected to increase sharply.
Even with harsh lockdown measures in place almost from day one of the first case being identified, the outbreak in Victoria is now the fastest growing of any Covid-19 cluster in Australia. At 1pm on Wednesday, the Royal Melbourne Hospital “pushed the button” on its “pandemic mode” operating model, which has already reached a critical point. The Saturday Paper has obtained a copy of the hospital’s “Covid-19 Operational Bed Plan” covering its city and Royal Park campus. It has reached stage 2 of the emergency preparations, with all eight ICU negative-pressure rooms full. A further three Covid-19 patients are receiving intensive care support in the hospital’s ICU “hot zone”.
“We are now sending away patients to other hospitals and not accepting patients from hospitals for whom we would normally be the first port of call,” an intensive care source at the Royal Melbourne Hospital tells The Saturday Paper.
“Elective cardiac surgery has not happened for two weeks, mostly due to the large numbers of ward staff furloughed. We may not have space for emergencies on the wards to come to ICU immediately – they may need to sit in the operating recovery room.
“We don’t know what we will do when the pandemic area is filled. The hospital is clearing wards now to make non-ICU Covid wards, as the dedicated Covid ward is full.”
Some of those who worked through Victoria’s second wave, and its aftermath, are so traumatised and exhausted that they may never come back. Certainly, some have refused. Last year, about 170 nursing and healthcare staff were trained to help expand the ICU capacity. They have been approached to serve again but only five have expressed an interest in returning.
“We were strained last year. However, in many ways this year is worse – we are all tired,” the health source says. “Last year we had an ‘oomph’ to get this done. Now we see this as a never-ending struggle. In the plan, you’ll see that ICU would expand to pods E, F and G. We don’t have the staff to be able to do that. It would take hundreds.”
The source says the emergency arrangements “must necessitate a reduction in usual care, but this has not been spelled out yet by the hospital executive”.
They continue: “I cried when I got home yesterday. We are all in for a very rough time, not just the staff but the community.”
This is not an isolated refrain. Paramedic Brett Simpson said he and his colleagues “have grave concerns” that there have already been avoidable deaths in NSW as a result of the system buckling.
Another says, “Without question, people have already died.”
For intensive care specialist Dr Holley, there is one way out of this crisis. “I truly encourage every single citizen to play their part and get vaccinated and follow the directive of the chief health officer in their state or jurisdiction,” he says. “That is how we stop this thing spreading. We need to do what we can to decrease demand on intensive care beds.”
I reada couple of par before it told me I could read no farther.
from Quotes…
Diplomacy
“I’m enjoying a week’s break in France. They’ve learned to live with Covid here not lurch from one damaging lockdown to another!”
Alexander DownerThe former Foreign minister enjoys a holiday in France. Most of the country has learnt to live with the virus, except for the 126,000 who didn’t and died.
Still, they are down to a mere 20,000 cases a day there now, perhaps even less.
“Another person familiar with the situation among paramedics, who asked not to be named, told The Saturday Paper the bed block, or ramping, of vehicles at Sydney hospitals is now so bad that hospital healthcare workers are X-raying patients in the back of ambulances and providing some early treatment before patients can be sorted into those cases urgent enough to warrant entry.”
I suspect that this is not correct. I doubt that any medical X-Ray equipment is portable for one, and I doubt the Radiation Safety Officer would allow that to happen, because it is an uncontrolled environment.
Maybe they mean that they are looking at patients in the back of ambulance, to assess whether or not the patient requires X-raying.
“Another person familiar with the situation among paramedics, who asked not to be named, told The Saturday Paper the bed block, or ramping, of vehicles at Sydney hospitals is now so bad that hospital healthcare workers are X-raying patients in the back of ambulances and providing some early treatment before patients can be sorted into those cases urgent enough to warrant entry.”
I suspect that this is not correct. I doubt that any medical X-Ray equipment is portable for one, and I doubt the Radiation Safety Officer would allow that to happen, because it is an uncontrolled environment.
Maybe they mean that they are looking at patients in the back of ambulance, to assess whether or not the patient requires X-raying.
They could ask the ambos. They could probably give a pretty good idea.
“Another person familiar with the situation among paramedics, who asked not to be named, told The Saturday Paper the bed block, or ramping, of vehicles at Sydney hospitals is now so bad that hospital healthcare workers are X-raying patients in the back of ambulances and providing some early treatment before patients can be sorted into those cases urgent enough to warrant entry.”
I suspect that this is not correct. I doubt that any medical X-Ray equipment is portable for one, and I doubt the Radiation Safety Officer would allow that to happen, because it is an uncontrolled environment.
Maybe they mean that they are looking at patients in the back of ambulance, to assess whether or not the patient requires X-raying.
I had my suspicions on that bit. we do have a portable x-ray machine in the local hospital.
“Another person familiar with the situation among paramedics, who asked not to be named, told The Saturday Paper the bed block, or ramping, of vehicles at Sydney hospitals is now so bad that hospital healthcare workers are X-raying patients in the back of ambulances and providing some early treatment before patients can be sorted into those cases urgent enough to warrant entry.”
I suspect that this is not correct. I doubt that any medical X-Ray equipment is portable for one, and I doubt the Radiation Safety Officer would allow that to happen, because it is an uncontrolled environment.
Maybe they mean that they are looking at patients in the back of ambulance, to assess whether or not the patient requires X-raying.
I had my suspicions on that bit. we do have a portable x-ray machine in the local hospital.
Hospital portable x ray machines are more like movable (on wheels) machines.
I reada couple of par before it told me I could read no farther.
from Quotes…
Diplomacy
“I’m enjoying a week’s break in France. They’ve learned to live with Covid here not lurch from one damaging lockdown to another!”
Alexander DownerThe former Foreign minister enjoys a holiday in France. Most of the country has learnt to live with the virus, except for the 126,000 who didn’t and died.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
Mum’s neighbour is still in hospital, in ICUAFAIK. His daughter who is about 10 years old has also been taken to hospital :(
Burwood LGA comprises just four suburbs — Burwood, Burwood Heights, Enfield and Enfield Heights — as well as parts of Croydon, Croydon Park and Strathfield, and is much smaller than the nearby Inner West and Canterbury-Bankstown LGAs of concern. Mr Chan said he understood Burwood was close to other areas with higher active case numbers. “We are also close to Campsie, Canterbury and all that. People usually come here for grocery shopping or food,” he said. “I think they only listed Burwood because we are surrounded by those places.”
It has recorded just 34 new COVID-19 cases in the past four weeks. But the local government area (LGA) of Burwood, in Sydney’s inner-west, is still being subject to the state’s most stringent restrictions.
Mr Chan said customers had told him case numbers were relatively low in Burwood compared to the inner-west or western suburbs. “We only have single-digit cases in a week.” He said it would be helpful if restrictions in Burwood were eased, but acknowledged it may not change the situation drastically. “Because of curfew, people are afraid to come out even for grocery shopping,” he said.
Burwood Mayor John Faker said he had been in discussions with the government to “show some compassion” and remove the council from the list, but it had fallen on deaf ears. He said it was disheartening to residents that the Inner West Council, which has recorded 222 cases in the past four weeks, was not considered an area of concern. “That’s why people are frustrated, it’s starting to feel like the government is discriminating against us,” Cr Faker said. “They’re starting to lose hope.”
Bill, who did not want to give his last name, lives in Glenmore Park, which is a suburb in the Penrith LGA that is not considered a high-risk area.
“My area is not a hotspot but it may as well be. aren’t that different.” “Our business in Burwood is open but we only work limited hours, we have to get a pass to come to work, all the fiddly stuff. Having to wear this mask is terrible.” He said he would support the government easing restrictions sooner for the fully vaccinated, before the 80 per cent double dose target. “If you’re fully vaccinated … slowly open up. Don’t keep us hostage waiting for the 80 per cent to get vaccinated. “People are going nuts, you can’t do anything.”
—
One, the antimask bullshit is stupid, but two, interesting how the fair go plays out. Especially given the reports we have from our contacts in Sydney how in actual high-incidence lockdown areas, there seems to be little compliance and little enforcement, while here you have reports of an area where cases are low, compliance is high, and… who the fuck knows.
“Another person familiar with the situation among paramedics, who asked not to be named, told The Saturday Paper the bed block, or ramping, of vehicles at Sydney hospitals is now so bad that hospital healthcare workers are X-raying patients in the back of ambulances and providing some early treatment before patients can be sorted into those cases urgent enough to warrant entry.”
I suspect that this is not correct. I doubt that any medical X-Ray equipment is portable for one, and I doubt the Radiation Safety Officer would allow that to happen, because it is an uncontrolled environment.
Maybe they mean that they are looking at patients in the back of ambulance, to assess whether or not the patient requires X-raying.
I had my suspicions on that bit. we do have a portable x-ray machine in the local hospital.
OK. If portable X-ray instruments are available, then their use as portables would be approved with an appropriate risk management strategy in place.
So let’s just say they (as they claim) are about 50% fully vaccinated, where does that put everyone¿
Taking the claimed numbers of 173 in intensive care and 137 of those unvaccinated, leaving 36 presumably vaccinated.
Since we have equal number (50%) of unvaccinated and vaccinated, we can directly compare these numbers for the level of protection.
137 / 36 = 3.8
As in, that “100% protection from severe disease and death” bullshit they lied to you about for the past 8 months¿ Yeah, in reality it’s a decrease in risk to 1/4, as in about a 75% protection. For now. Nice.
The rate of Covid-19 hospitalisations in New South Wales is being reported at one-third of the real figure, with the actual numbers being masked by a decision to only report those who end up in medical facilities, and not the thousands receiving care under the state’s “hospital in the home” arrangements.
On Tuesday, Premier Gladys Berejiklian said the “most recent figure I have for the rate of hospitalisation was 5.5 per cent in terms of cases converting to hospitalisation”. The real figure, however, is about 15 per cent, according to medical experts and a briefing provided to national cabinet.
On Thursday, the state reported almost 1000 people with Covid-19 were in hospital and 160 of those were receiving the most complex form of healthcare in intensive care units.
But that figure leaves out almost 1700 people who are receiving hospital-grade care for coronavirus in their own homes in NSW. Most of those are being monitored by staff from the swamped Westmead Hospital in the state’s Western Sydney Local Health District. Under these arrangements, patients who would otherwise be on the hospital ward are instead given oxygen and other support at home with scheduled visits from hospital staff.
At least eight people in the state have died at home since the Delta outbreak began. Some, who were being given home care, deteriorated so quickly from mild illness to death that there was no time for even an ambulance to be called. The coroner is investigating these deaths.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
The CHRIS platform, developed last year in response to Covid-19, is the same platform used to prepare briefings for national cabinet. In just three weeks the number of staffed ICU beds in NSW has actually fallen by nine.
In advice prepared for national cabinet, hospital demand in all states and territories was forecast using a “transition ratio” from active Covid-19 case to hospitalisation. In the document, obtained by The Saturday Paper, political leaders were told this ratio was calculated by dividing the number of individuals requiring hospitalisation by the number of active cases in the week before. By this method, the hospitalisation ratio is 0.16 or 16 per cent.
Garvan Institute of Medical Research executive director Professor Christopher Goodnow told staff in a private briefing that “hospitalisation is tracking around 15 per cent in the current NSW outbreak”.
These figures are important because health system workers who have spoken with The Saturday Paper believe clinical care is already being compromised in the NSW outbreak and may have already caused the death of people who might otherwise have been saved.
Australian and New Zealand Intensive Care Society president Dr Anthony Holley, whose organisation is advising national cabinet, is blunt.
“The imposition of Covid on the system and the challenge and the stress that is in place cannot and should not be underestimated,” he told The Saturday Paper. “There will be implications. I am deeply concerned and would never underestimate the situation, but I am also confident the professionalism of the front-line workers is such that they will minimise those implications.”
Intensive care paramedic and delegate for the NSW branch of the Australian Paramedics Association Brett Simpson says the ambulance service in the state has already moved beyond its capacity to cope.
Last year, about 170 nursing and healthcare staff were trained to help expand the ICU… only five have expressed an interest in returning.
“You can increase ICU capacity all you want but if we can’t get you to the hospital alive then what’s the point? The ambulance service is not coping in any sense of the word. What we are seeing at the moment are outrageous response times,” he says.
“The worst example I was given last week is a crew from Bateau Bay on the Central Coast having to run lights and sirens to South Granville in Sydney for a house of people with Covid who were all short of breath. Ordinarily, that is a 1.5-hour drive. The distance is 100 kilometres. It is far from an isolated incident. Crews are having to drive half an hour to reach a patient in cardiac arrest,” Simpson said.
Time and again healthcare workers have made the point to this newspaper that it is not just Covid-19 patients who are affected by the system pressure. Everyone who needs medical attention is at risk.
In Liverpool, in the South Western Sydney Local Health District, a 50-year-old man fell three metres from the roof of his house and suffered severe leg injuries, including a horrific “degloving” of his lower left leg.
“After half an hour, when the ambulance just simply hadn’t turned up, his wife dragged him to the car and drove him to Liverpool Hospital on her own – and this is happening more and more and more often,” Simpson says. “The entire health system, despite whatever is happening with Covid and bed block , people are still having heart attacks, they are still having strokes, car and truck accidents, industrial accidents.
“At the moment we are seeing hot jobs sitting in the queue waiting over an hour for an ambulance even to be dispatched on it, let alone get a paramedic crew arriving on the scene.”
By Simpson’s telling, the hospital emergency department network is so finely calibrated that when one becomes overwhelmed, the spillover affects another and another. They fall like dominoes.
The Saturday Paper has obtained a new “patient allocation matrix” for emergency admissions in NSW hospitals that dictates what facilities are available for certain categories of illness. On August 25, the document was circulated to paramedics with two new categories: confirmed Covid-19 and suspected Covid-19.
Of the 46 hospitals – mostly public, with some private – in the local health districts covering the Newcastle–Hunter region, the Central Coast, all of Greater Sydney and Wollongong–Shoalhaven, fewer than half, or 19, are accepting confirmed Covid-19 patients.
In the Western Sydney Local Health District, only Westmead is listed as accepting confirmed cases. Auburn, Blacktown and Mount Druitt will not. Similarly, in the Nepean Blue Mountains Local Health District, only Nepean Hospital is taking admissions for the infection. In south-western Sydney, Liverpool and Campbelltown hospitals are taking Covid-19 patients but Bankstown, Fairfield and Bowral are not.
The only health district so far open for all Covid-19 confirmed and suspected cases is the Northern Sydney region. On Tuesday night, ambulance cars trying to get patients into Westmead, but facing severe bed block, were told to go to the Northern Beaches Hospital almost 35 kilometres away.
As hospitals fill, the domino-effect described by Simpson will become more pronounced.
Another person familiar with the situation among paramedics, who asked not to be named, told The Saturday Paper the bed block, or ramping, of vehicles at Sydney hospitals is now so bad that hospital healthcare workers are X-raying patients in the back of ambulances and providing some early treatment before patients can be sorted into those cases urgent enough to warrant entry.
In the final week of August, major hospitals across the network erected tents at their entrances to help triage Covid-19 patients. But their use differs between each facility. At Royal Prince Alfred Hospital in Camperdown, for example, the mini field hospital has spaced seating for about six patients with Covid-19 to be assessed and treated while waiting for admission. At Westmead, one of the largest hospitals in Australia, the Covid tents are being used to assess patients and offer very basic initial treatment, such as fluids or a Covid-19 test, before sending them back into the ambulances in which they came.
A senior health official said there was a delay in erecting the tents because authorities were worried it would be a “bad look” if the public saw hospital staff in full protective equipment treating people in makeshift marquees. This reluctance made the ambulance bed block issue even worse.
Last weekend, 17 ambulances were bed blocked at Westmead Hospital. As another source says: “That has never happened at any time in the history of the state.”
On Wednesday, Gladys Berejiklian told reporters that “the worst hospitalisation rate is likely to be in October”.
She said: “The most recent advice that I have received is that case numbers are likely to continue to rise in the next few weeks. We know that there is always a lag between when someone gets ill and when they end up in hospital and we anticipate that given where the case numbers are, and given the rate of vaccination, that the highest rate of hospitalisation will occur at some stage in October.”
Nursing staff and doctors are worried about what happens between now and then. The health network is already fragile and so finely calibrated that the pressure threatens to cascade without some intervention.
A source familiar with the operation of Lismore Base Hospital in the state’s northern rivers district says the facility, which has been designated the Covid-19 hospital for the Northern NSW Local Health District, has just four ICU beds. Currently, all of these are occupied by patients without Covid-19.
“As it stands, there are only 4.5 full-time ICU nurses to cover 24/7 care, less than half of the staffing that is needed to cover the weekly roster,” the source says. “Two ICU supervising doctors out of four have been redeployed to Sydney and there is currently no formal agreement between NSW and Queensland regarding what happens to all the northern NSW residents that rely on medical care across the border.
“It is a total shitshow. Paramedics, nurses and other operational staff cannot cross the border with ease at the moment and all key services are having major staffing issues.”
Where once a health crisis in one part of Australia could be met with support from other jurisdictions, the Delta variant represents a risk that has never before been seen.
On Wednesday, Victorian Premier Daniel Andrews announced a dramatic shift in the state’s thinking about Covid-19. The Delta variant outbreak that was seeded from NSW can no longer be controlled, he said.
“We have thrown everything at it, but it is now clear to us that we are not going to drive these numbers down, they’re instead going to increase,” he conceded at a press conference.
Behind the scenes, the situation is more severe than even that update allowed. Data from the Critical Health Resource Information System shows that 391 of the 429 currently staffed ICU beds in Victoria – 91 per cent – are occupied. Of these, 20 are being used for Covid-19 patients – but that number is expected to increase sharply.
Even with harsh lockdown measures in place almost from day one of the first case being identified, the outbreak in Victoria is now the fastest growing of any Covid-19 cluster in Australia. At 1pm on Wednesday, the Royal Melbourne Hospital “pushed the button” on its “pandemic mode” operating model, which has already reached a critical point. The Saturday Paper has obtained a copy of the hospital’s “Covid-19 Operational Bed Plan” covering its city and Royal Park campus. It has reached stage 2 of the emergency preparations, with all eight ICU negative-pressure rooms full. A further three Covid-19 patients are receiving intensive care support in the hospital’s ICU “hot zone”.
“We are now sending away patients to other hospitals and not accepting patients from hospitals for whom we would normally be the first port of call,” an intensive care source at the Royal Melbourne Hospital tells The Saturday Paper.
“Elective cardiac surgery has not happened for two weeks, mostly due to the large numbers of ward staff furloughed. We may not have space for emergencies on the wards to come to ICU immediately – they may need to sit in the operating recovery room.
“We don’t know what we will do when the pandemic area is filled. The hospital is clearing wards now to make non-ICU Covid wards, as the dedicated Covid ward is full.”
Some of those who worked through Victoria’s second wave, and its aftermath, are so traumatised and exhausted that they may never come back. Certainly, some have refused. Last year, about 170 nursing and healthcare staff were trained to help expand the ICU capacity. They have been approached to serve again but only five have expressed an interest in returning.
“We were strained last year. However, in many ways this year is worse – we are all tired,” the health source says. “Last year we had an ‘oomph’ to get this done. Now we see this as a never-ending struggle. In the plan, you’ll see that ICU would expand to pods E, F and G. We don’t have the staff to be able to do that. It would take hundreds.”
The source says the emergency arrangements “must necessitate a reduction in usual care, but this has not been spelled out yet by the hospital executive”.
They continue: “I cried when I got home yesterday. We are all in for a very rough time, not just the staff but the community.”
This is not an isolated refrain. Paramedic Brett Simpson said he and his colleagues “have grave concerns” that there have already been avoidable deaths in NSW as a result of the system buckling.
Another says, “Without question, people have already died.”
For intensive care specialist Dr Holley, there is one way out of this crisis. “I truly encourage every single citizen to play their part and get vaccinated and follow the directive of the chief health officer in their state or jurisdiction,” he says. “That is how we stop this thing spreading. We need to do what we can to decrease demand on intensive care beds.”
So let’s just say they (as they claim) are about 50% fully vaccinated, where does that put everyone¿
Taking the claimed numbers of 173 in intensive care and 137 of those unvaccinated, leaving 36 presumably vaccinated.
Since we have equal number (50%) of unvaccinated and vaccinated, we can directly compare these numbers for the level of protection.
137 / 36 = 3.8
As in, that “100% protection from severe disease and death” bullshit they lied to you about for the past 8 months¿ Yeah, in reality it’s a decrease in risk to 1/4, as in about a 75% protection. For now. Nice.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
Mum’s neighbour is still in hospital, in ICUAFAIK. His daughter who is about 10 years old has also been taken to hospital :(
Shit. How’s your mother?
Mum and her husband had their Covid tests and they came back negative, but geez, when her husband told me they delayed being tested as they needed to stock up at Woolies first, just in case, I was not impressed, especially as I had offered to bring them supplies if they needed some. It’s no wonder those LGAs of concern are still LGAs of concern :(
“Conflicting” yeah we probably won’t take life-saving advice from the crowd that think it’s worth sacrificing 250000 people to a preventable disease just so The Economy Can Grow dramatically (+1000000000000%) from its deep recession (-100%) caused by pandemic failure.
So let’s just say they (as they claim) are about 50% fully vaccinated, where does that put everyone¿
Taking the claimed numbers of 173 in intensive care and 137 of those unvaccinated, leaving 36 presumably vaccinated.
Since we have equal number (50%) of unvaccinated and vaccinated, we can directly compare these numbers for the level of protection.
137 / 36 = 3.8
As in, that “100% protection from severe disease and death” bullshit they lied to you about for the past 8 months¿ Yeah, in reality it’s a decrease in risk to 1/4, as in about a 75% protection. For now. Nice.
Closer to 70% have at least the first dose.
Dunno, we thought they said you need both because with only 1 it’s like 10% effective… we just picked something in between the first and second dose counts from this.
Mum’s neighbour is still in hospital, in ICUAFAIK. His daughter who is about 10 years old has also been taken to hospital :(
Shit. How’s your mother?
Mum and her husband had their Covid tests and they came back negative, but geez, when her husband told me they delayed being tested as they needed to stock up at Woolies first, just in case, I was not impressed, especially as I had offered to bring them supplies if they needed some. It’s no wonder those LGAs of concern are still LGAs of concern :(
“Another person familiar with the situation among paramedics, who asked not to be named, told The Saturday Paper the bed block, or ramping, of vehicles at Sydney hospitals is now so bad that hospital healthcare workers are X-raying patients in the back of ambulances and providing some early treatment before patients can be sorted into those cases urgent enough to warrant entry.”
I suspect that this is not correct. I doubt that any medical X-Ray equipment is portable for one, and I doubt the Radiation Safety Officer would allow that to happen, because it is an uncontrolled environment.
Maybe they mean that they are looking at patients in the back of ambulance, to assess whether or not the patient requires X-raying.
I had my suspicions on that bit. we do have a portable x-ray machine in the local hospital.
OK. If portable X-ray instruments are available, then their use as portables would be approved with an appropriate risk management strategy in place.
So my earlier comment is likely wrong.
Surely treating these highly infectious airborne pathogen patients outside is a more sensible thing to do anyway, we’ve had to go to emergency departments before, they look pretty boxed in and the smells can be pretty lingering so it doesn’t really seem like they’re very well set up to deal with any real pandemics.
I reada couple of par before it told me I could read no farther.
from Quotes…
Diplomacy
“I’m enjoying a week’s break in France. They’ve learned to live with Covid here not lurch from one damaging lockdown to another!”
Alexander DownerThe former Foreign minister enjoys a holiday in France. Most of the country has learnt to live with the virus, except for the 126,000 who didn’t and died.
I declare Alexander Downer to be a fuckwit. Short and sharp lockdowns are not really as economically damaging as the free market jihadists make out. They are an inconvenience for sure, but they are followed by a quick rebound back to normal once zero Covid has been achieved and restrictions are lifted.
“Conflicting” yeah we probably won’t take life-saving advice from the crowd that think it’s worth sacrificing 250000 people to a preventable disease just so The Economy Can Grow dramatically (+1000000000000%) from its deep recession (-100%) caused by pandemic failure.
‘Conflicting’ was my take on an article and headline that I thought was so cut and dried.
“Conflicting” yeah we probably won’t take life-saving advice from the crowd that think it’s worth sacrificing 250000 people to a preventable disease just so The Economy Can Grow dramatically (+1000000000000%) from its deep recession (-100%) caused by pandemic failure.
‘Conflicting’ was my take on an article and headline that I thought was so cut and dried.
The Saturday Paper has also been provided access to the nation’s Critical Health Resource Information System (CHRIS), which provides real-time data on the use of intensive care beds in every state and territory hospital network. On Thursday, 80 per cent or 689 of the 855 staffed ICU beds in NSW were full. Of these, 170 – or one-quarter of the occupied beds – are being used to treat Covid-19 patients. The situation in Victoria is worse. More than 90 per cent of ICU beds are full there. Hospitals are struggling to encourage nurses who worked in last year’s outbreak to help again.
A bit of pea and thimble trick there. There’s 23 patients with the rona in ICU in Victoria.
The whole article is nuts.
He actually does go to the trouble of pointing this out, but near the end of the article.
From the link Bogsnorkler provided, they mention delivering oxygen at home¿ Sounds like NSW is really fucked, at least if we’re reading the following right.
so bite us, and things may have changed since then, but when it says
Therapeutics of hospital in the home
There are 3 major therapeutic tools available to hospital in the home units (HHUs).
Intravenous therapy
Intravenous therapy mainly involves antibiotics, but also corticosteroids, chemotherapeutic agents, blood and blood products, crystalloids and inotropes.
Anticoagulation
Subcutaneous low molecular weight heparins can be given at home to patients with uncomplicated deep venous thrombosis.
Dressings
Complex wounds including postoperative wounds, wound breakdown and burns can be managed using expensive dressings that generally require hospitalisation
we seem to have missed the part where it says “oxygen” and then they have this
Patient selection
Patients are referred from inpatient wards or the emergency department, and are assessed by a HHU nurse. Choosing appropriate patients is a challenge. Selection criteria need to be applied with experience and flexibility, but should include:
– a patient who would normally require hospital care for a stable condition who is unlikely to need emergency interventions. Fever and moderate pain (not requiring opioid analgesia) are not contraindications
which makes us wonder, when they’re finding people often the protestors and antimaskers and antilockdowners randomly dying at home, does that qualify as “stable condition who is unlikely to need emergency interventions“¿
He actually does go to the trouble of pointing this out, but near the end of the article.
From the link Bogsnorkler provided, they mention delivering oxygen at home¿ Sounds like NSW is really fucked, at least if we’re reading the following right.
so bite us, and things may have changed since then, but when it says
Therapeutics of hospital in the home
There are 3 major therapeutic tools available to hospital in the home units (HHUs).
Intravenous therapy
Intravenous therapy mainly involves antibiotics, but also corticosteroids, chemotherapeutic agents, blood and blood products, crystalloids and inotropes.
Anticoagulation
Subcutaneous low molecular weight heparins can be given at home to patients with uncomplicated deep venous thrombosis.
Dressings
Complex wounds including postoperative wounds, wound breakdown and burns can be managed using expensive dressings that generally require hospitalisation
we seem to have missed the part where it says “oxygen” and then they have this
Patient selection
Patients are referred from inpatient wards or the emergency department, and are assessed by a HHU nurse. Choosing appropriate patients is a challenge. Selection criteria need to be applied with experience and flexibility, but should include:
– a patient who would normally require hospital care for a stable condition who is unlikely to need emergency interventions. Fever and moderate pain (not requiring opioid analgesia) are not contraindications
which makes us wonder, when they’re finding people often the protestors and antimaskers and antilockdowners randomly dying at home, does that qualify as “stable condition who is unlikely to need emergency interventions“¿
When mum was on her last legs she was at home for a goodly while with oxygen. the biggest bit seemed to be convincing them that she had really given up smoking.
“Conflicting” yeah we probably won’t take life-saving advice from the crowd that think it’s worth sacrificing 250000 people to a preventable disease just so The Economy Can Grow dramatically (+1000000000000%) from its deep recession (-100%) caused by pandemic failure.
‘Conflicting’ was my take on an article and headline that I thought was so cut and dried.
grrrr wasn’t
Nah all fair it’s just a bit like with Sverige, USUK, NSWuhan … when some bunch of dudes have demonstrably fkd up their healthcare, then we decide not to listen closely to what they have to claim about healthcare from then on.
We mean when was the last time privileged arseholes rocked up at their local hospital in Australia and demanded a level of healthcare comparable to Brazil or South Africa or Bangladesh¿
(Actually they must be experts at treating TB or malaria or stuff like that though.)
He actually does go to the trouble of pointing this out, but near the end of the article.
From the link Bogsnorkler provided, they mention delivering oxygen at home¿ Sounds like NSW is really fucked, at least if we’re reading the following right.
so bite us, and things may have changed since then, but when it says
Therapeutics of hospital in the home
There are 3 major therapeutic tools available to hospital in the home units (HHUs).
Intravenous therapy
Intravenous therapy mainly involves antibiotics, but also corticosteroids, chemotherapeutic agents, blood and blood products, crystalloids and inotropes.
Anticoagulation
Subcutaneous low molecular weight heparins can be given at home to patients with uncomplicated deep venous thrombosis.
Dressings
Complex wounds including postoperative wounds, wound breakdown and burns can be managed using expensive dressings that generally require hospitalisation
we seem to have missed the part where it says “oxygen” and then they have this
Patient selection
Patients are referred from inpatient wards or the emergency department, and are assessed by a HHU nurse. Choosing appropriate patients is a challenge. Selection criteria need to be applied with experience and flexibility, but should include:
– a patient who would normally require hospital care for a stable condition who is unlikely to need emergency interventions. Fever and moderate pain (not requiring opioid analgesia) are not contraindications
which makes us wonder, when they’re finding people often the protestors and antimaskers and antilockdowners randomly dying at home, does that qualify as “stable condition who is unlikely to need emergency interventions“¿
When mum was on her last legs she was at home for a goodly while with oxygen. the biggest bit seemed to be convincing them that she had really given up smoking.
but is that for emphysema as opposed to some explosive coronavirus that’s putting people in ICU within 5 days, like
another old article so we’ll be all tooth marks soon but here
The use of oxygen therapy, especially at home, for patients with chronic hypoxaemia has been the subject of more discussion. Guidelines have been developed by the Thoracic Society of Australia and New Zealand to limit the inappropriate use of what can be a valuable but expensive form of treatment.1
doesn’t say it’s the only reason for it though
(we’re sure oxygen at home isn’t a new thing but seems like just doling it out to COVID-19 patients is as much a political manoeuvre as a necessary health provision one)
From the link Bogsnorkler provided, they mention delivering oxygen at home¿ Sounds like NSW is really fucked, at least if we’re reading the following right.
so bite us, and things may have changed since then, but when it says
Therapeutics of hospital in the home
There are 3 major therapeutic tools available to hospital in the home units (HHUs).
Intravenous therapy
Intravenous therapy mainly involves antibiotics, but also corticosteroids, chemotherapeutic agents, blood and blood products, crystalloids and inotropes.
Anticoagulation
Subcutaneous low molecular weight heparins can be given at home to patients with uncomplicated deep venous thrombosis.
Dressings
Complex wounds including postoperative wounds, wound breakdown and burns can be managed using expensive dressings that generally require hospitalisation
we seem to have missed the part where it says “oxygen” and then they have this
Patient selection
Patients are referred from inpatient wards or the emergency department, and are assessed by a HHU nurse. Choosing appropriate patients is a challenge. Selection criteria need to be applied with experience and flexibility, but should include:
– a patient who would normally require hospital care for a stable condition who is unlikely to need emergency interventions. Fever and moderate pain (not requiring opioid analgesia) are not contraindications
which makes us wonder, when they’re finding people often the protestors and antimaskers and antilockdowners randomly dying at home, does that qualify as “stable condition who is unlikely to need emergency interventions“¿
When mum was on her last legs she was at home for a goodly while with oxygen. the biggest bit seemed to be convincing them that she had really given up smoking.
but is that for emphysema as opposed to some explosive coronavirus that’s putting people in ICU within 5 days, like
another old article so we’ll be all tooth marks soon but here
The use of oxygen therapy, especially at home, for patients with chronic hypoxaemia has been the subject of more discussion. Guidelines have been developed by the Thoracic Society of Australia and New Zealand to limit the inappropriate use of what can be a valuable but expensive form of treatment.1
doesn’t say it’s the only reason for it though
(we’re sure oxygen at home isn’t a new thing but seems like just doling it out to COVID-19 patients is as much a political manoeuvre as a necessary health provision one)
Also Mum was sort of stable and had a bunch of people looking out for her and a resident alcoholic in case someone competant needed to be paged. I gather covid + oxygen patients need quite a bit of nursing from friends and family.
‘Conflicting’ was my take on an article and headline that I thought was so cut and dried.
grrrr wasn’t
Nah all fair it’s just a bit like with Sverige, USUK, NSWuhan … when some bunch of dudes have demonstrably fkd up their healthcare, then we decide not to listen closely to what they have to claim about healthcare from then on.
We mean when was the last time privileged arseholes rocked up at their local hospital in Australia and demanded a level of healthcare comparable to Brazil or South Africa or Bangladesh¿
(Actually they must be experts at treating TB or malaria or stuff like that though.)
Nah all fair it’s just a bit like with Sverige, USUK, NSWuhan … when some bunch of dudes have demonstrably fkd up their healthcare, then we decide not to listen closely to what they have to claim about healthcare from then on.
We mean when was the last time privileged arseholes rocked up at their local hospital in Australia and demanded a level of healthcare comparable to Brazil or South Africa or Bangladesh¿
(Actually they must be experts at treating TB or malaria or stuff like that though.)
McGowan wants at least 80 per cent of eligible West Australians vaccinated before he will set a date for bringing down the hard border, which will likely be a couple of months after that target is reached. Currently, WA is on track to reach 80 per cent double-dose vaccination in early December for people aged 16 and over. But the WA government will include children aged 12 and over in its vaccination threshold, which is another deviation from the national plan, and it is not yet clear when that target will be reached. “If we get to 80 per cent two dose vaccinated … my aim would be to get significantly above that … and then set a date,” Mr McGowan said. “And when you set the date, that will incentivise people to go and get vaccinated.” Mr McGowan said the Doherty Institute modelling indicated that opening WA’s border at 70 per cent vaccination would be disastrous for the state, leading to five deaths per day. “The idea that we deliberately bring down the border at 70 per cent, infect our citizens in large numbers and then have to lock down our community, and five people a day die, was somehow a good idea, is just wrong,” he said.
Acting Premier Jeremy Rockliff also said, “we want every Tasmanian to have the opportunity to be vaccinated”, and that the threshold to reopen included those in the 12-16 age group.
Palaszczuk left no doubt about her unease about opening up before children were vaccinated, saying: “Unless there is an answer on how these young people are going to be vaccinated, you are putting the most vulnerable population at risk.” “I am asking very simple questions here of Scott Morrison and from the National Cabinet,” Palaszczuk said on Thursday. “It is only fair and reasonable we have a constructive debate in this country and, rather than picking fights and attacks, let’s have a decent, educated conversation. And there is nothing wrong about asking decent questions about the safety of families.”
Worldwide, no vaccine has been broadly approved for children under 12, which adds to the difficulty of ensuring schools can reopen safely.
Morrison, for his part, is writing to Australians aged over 60 who have yet to come forward for the AstraZeneca vaccine.
“We saw the material that has just been rife on the internet being used by people to injure Aboriginal people intentionally,” Mr McLean said.
—
Actually, Marketing seems to have the smartest idea here, we’re not exactly 60 years old but we’d be so revolted by the idea of getting a letter from the arsehole that we’d probably book in 50 times just to avoid it.
toughen up you cowards, it’s just a mild head cold
had a quick look, got the gist of flavor about it, so won’t continue
I will say that some of the very important practices used in hospitals have been done (previously of some States) extremely successfully by the broader community so hospitals don’t become covid-central and overwhelmed, and some of the media have been part of, or lent to a program to release covid, the release of a biological hazard
Berejiklian says NSW will ‘certainly not have a statewide lockdown ever again’ once 80 per cent vaccination is reached
Ms Berejiklian says life will look better when 80 per cent of the population has had two doses of a COVID vaccine.
“I know I sound like a broken record, but with good reason because when we get those vaccination rates, life will look better and feel better and we certainly will not have to have a statewide lockdown ever again when we hit the 80 per cent double dose vaccination rates which is what we’re looking forward to.”
———————————————————————————————————————————-
I can’t remember – has NSW actually done a full statewide lockdown either this year or last year?
Berejiklian says NSW will ‘certainly not have a statewide lockdown ever again’ once 80 per cent vaccination is reached
Ms Berejiklian says life will look better when 80 per cent of the population has had two doses of a COVID vaccine.
“I know I sound like a broken record, but with good reason because when we get those vaccination rates, life will look better and feel better and we certainly will not have to have a statewide lockdown ever again when we hit the 80 per cent double dose vaccination rates which is what we’re looking forward to.”
———————————————————————————————————————————-
I can’t remember – has NSW actually done a full statewide lockdown either this year or last year?
Berejiklian says NSW will ‘certainly not have a statewide lockdown ever again’ once 80 per cent vaccination is reached
Ms Berejiklian says life will look better when 80 per cent of the population has had two doses of a COVID vaccine.
“I know I sound like a broken record, but with good reason because when we get those vaccination rates, life will look better and feel better and we certainly will not have to have a statewide lockdown ever again when we hit the 80 per cent double dose vaccination rates which is what we’re looking forward to.”
———————————————————————————————————————————-
I can’t remember – has NSW actually done a full statewide lockdown either this year or last year?
Berejiklian says NSW will ‘certainly not have a statewide lockdown ever again’ once 80 per cent vaccination is reached
Ms Berejiklian says life will look better when 80 per cent of the population has had two doses of a COVID vaccine.
“I know I sound like a broken record, but with good reason because when we get those vaccination rates, life will look better and feel better and we certainly will not have to have a statewide lockdown ever again when we hit the 80 per cent double dose vaccination rates which is what we’re looking forward to.”
———————————————————————————————————————————-
I can’t remember – has NSW actually done a full statewide lockdown either this year or last year?
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
They look like dedicated caravan spaces – they will have water and electricity at those spots.
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
They look like dedicated caravan spaces – they will have water and electricity at those spots.
It’s the showgrounds according to the story. But I suppose you’re right. Stuff will happen in measurements it normally happens in.
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
IDGI.
large families and extended family, a lot of people per house and some significant unmanageable mixing, in houses and between houses, sociability
lot of unvaccinated people hiding form vaccinated people that spread the contagion, were hiding from the aggression vaccinators
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
IDGI.
large families and extended family, a lot of people per house and some significant unmanageable mixing, in houses and between houses, sociability
lot of unvaccinated people hiding form vaccinated people that spread the contagion, were hiding from the aggression vaccinators
Covid outbreak, predominantly indigenous and minimal vaccination as it wasn’t available.
And being an outbreak in a small population the stats are bad.
More than 13 per cent of the community of 800 people has COVID
When you live in large and extended family groups, one person tests positive and is told to stay at home for 14 days…guess what happens to everyone else in the house. The virus just rolls along through until it’s got everyone. And that extends the issue.
They have a lot of room. I wonder why they aren’t using it…
IDGI.
large families and extended family, a lot of people per house and some significant unmanageable mixing, in houses and between houses, sociability
lot of unvaccinated people hiding form vaccinated people that spread the contagion, were hiding from the aggression vaccinators
OK this is pretty bloody important so all yous wait the fuck up.
Apparently when they want to quarantine a bunch of First Nations People in remote NSW, they’re able to find vast expanses of land and mobile facilities to just bring in at the snap of some fingers, enabling people to enjoy a holiday in air gapped separate living spaces, without deep concern for proximity to advanced quaternary medical services¿
But if they were meant to quarantine a bunch of privileged First World Pricks returning from corruption parties overseas, then there was no fucking way for 20 months that they could set anything up that would work¿ It was so difficult that the quarantine systems they did use, failed¿ If they hadn’t failed, then we wouldn’t be quarantining our First Nations People in remote NSW in caravans¿
Oh yeah¿ Bet you the majority of the 5000000 (undercount) COVID-19 fatalities to date were in full support of vaccinations¡
that was going to be my next question.. how many people who are vaccination supporters died? has anyone who has been vaccinated died? also are these people dying OF Covid or WITH covid?
Wilcannia gets COVID repreive as motorhomes arrive to form isolation hub
https://www.abc.net.au/news/2021-09-05/nsw-wilcannia-motorhomes-isolation-hub/100434846
They have a lot of room. I wonder why they aren’t using it…
Oh yeah¿ Bet you the majority of the 5000000 (undercount) COVID-19 fatalities to date were in full support of vaccinations¡
that was going to be my next question.. how many people who are vaccination supporters died? has anyone who has been vaccinated died? also are these people dying OF Covid or WITH covid?
Unsure, as that site I linked to only listed those who we vocally anti vacccination.
Oh yeah¿ Bet you the majority of the 5000000 (undercount) COVID-19 fatalities to date were in full support of vaccinations¡
yeah don’t like that site much, given a lot of people were really deprived one of the basic purposes of borders(exercised by governments), which is to stop or at least slow down a threat, in this case the serious threat was and is a biological hazard, a contagion, covid
and I note, to give it a more local dimension, here in this State right now I guess it is truck drivers, largely vaccinated probably, originating from the superspreader State
point being vaccinated people can and do spread covid, under license of being vaccinated, people do, then you have another contagion of people ‘doing the right thing’, a sort of impunity
Probably true. But this requires foresight and planning; and more importantly: the spending of public money on stockpiling for something that only “might” happen.
Hard to know right, it’s outdoors, there are some masks, some not, and it would require presence of the virus at those particular sites … but it’s B.1.617.2 which does get pretty transmissible.
Hard to know right, it’s outdoors, there are some masks, some not, and it would require presence of the virus at those particular sites … but it’s B.1.617.2 which does get pretty transmissible.
The Future For Roentgenium Standard Enlighened New South Wuhan
Dozens of positive COVID-19 tests discovered outside the grounds of a music festival in the United Kingdom have shocked festival-goers.
Reading Festival is one of the U.K.‘s biggest festivals and it took place last weekend, headlined by Stormzy and Liam Gallagher with an estimated 90,000 people in attendance.
Ticket holders were required to provide proof of double vaccination or a negative lateral flow test to gain entry. Once inside, revelers were then required to take a new lateral flow test every 72 hours.
TikTok videos from the event also purport to show positive lateral flow tests discarded on the ground.
In a statement on Friday, after days of speculation, the Joint Committee on Vaccination and Immunisation (JCVI) said that while the health gains from vaccinating the entire age group were greater than the risks, “the margin of benefit is considered too small to support universal vaccination of healthy 12- to 15-year-olds at this time”.
However, in a tacit invitation to overrule its own recommendation the JCVI stressed that because its remit does not include wider issues such as disruption to schools, ministers could consider seeking separate advice on this, an unprecedented suggestion by the organisation.
So this JCVI recommendation, was it put forward by Robert S. Mueller, III¿
1- The figure for full vaccination in NSW.
2- This shows what is behind the rise of those yellow dots. They are mostly areas of concern in NSW.
3- This one shows this is not just income, the correlation is visible with SEIFA for all AUS.
not sure I really understand what the story is here.. I would expect the national plan should be open to change as underlying circumstances change..
I believe it is the different messages from stuart and morrison. Personally i agree with you in that with new data plans should change.
I saw the interview and what he said made perfect sense… the problem for me is that there is no clear change management process.. I mean, FFS, some of this stuff is risk management 101.
Not all persons recovering from severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection develop SARS-CoV-2–specific antibodies. We show that nonseroconversion is associated with younger age and higher reverse transcription PCR cycle threshold values and identify SARS-CoV-2 viral loads in the nasopharynx as a major correlate of the systemic antibody response.
imagine if the people that “don’t get serious disease” don’t get serious protection, or the “longer lasting protection”* only applies to a few people, or more generally, if flock immunity through mass infection … isn’t
*: coming but not so soon, to a benzocaine phallus-mask near you
However, more recent studies have shown that seroconversion rates are surprisingly variable (6–10). For example, a multicenter study from Israel reported that 5% of participants remained seronegative despite a positive test result on a nasal swab specimen (6). In contrast, a seroprevalence study from New York found that 20% of persons with a positive RT-PCR test result did not seroconvert (8). Another study from Germany reported that 85% of confirmed infected COVID-19 contacts failed to develop antibodies (9).
I had a day of flu symptoms after the first AZ jab, but no pain or numbness at the site of the jab.s
Next one on the 23rd of this month.
I froze for a couple of days and I had a huge reaction at the site of the jab that hung around for over a week.
Really? In Tassie in winter?
I got the chills and they multiplied. I burned lots of firewood and filled the ot water bottle many times. And spent most of the time in bed with an extra blanket.l
The Prime Minister travelled to Sydney over the weekend, despite the COVID-19 lockdowns in the ACT and New South Wales.
Scott Morrison spent all of yesterday, Father’s Day, in his home city.
He returned to Canberra this morning, ahead of a national summit on women’s safety.
His office says the PM abided by health guidelines and was approved by ACT health authorities to return to the nation’s capital for work.
“I’m really glad the Prime Minister got to spend Father’s Day with his two girls,” said Federal Labor frontbencher Kristina Keneally.
“I’m sure that meant a great deal to him.”
However, Senator Keneally added that many other families around Australia would also have liked to be reunited over the weekend.
“There are tens of thousands of people separated right now and I’m sure on Father’s Day those families would have liked to see their children too,” she said.
“We’re in this situation because the Prime Minister hasn’t got the vaccine rollout working and didn’t set up a fit for purpose quarantine system. Now that he’s back in Canberra I hope he’s spending time making sure Australians get vaccinated.
“No one wants to go through Christmas as they just did Father’s Day.”
Mr Morrison is likely to travel back to Sydney early this week.
The Prime Minister travelled to Sydney over the weekend, despite the COVID-19 lockdowns in the ACT and New South Wales.
Scott Morrison spent all of yesterday, Father’s Day, in his home city.
He returned to Canberra this morning, ahead of a national summit on women’s safety.
His office says the PM abided by health guidelines and was approved by ACT health authorities to return to the nation’s capital for work.
“I’m really glad the Prime Minister got to spend Father’s Day with his two girls,” said Federal Labor frontbencher Kristina Keneally.
“I’m sure that meant a great deal to him.”
However, Senator Keneally added that many other families around Australia would also have liked to be reunited over the weekend.
“There are tens of thousands of people separated right now and I’m sure on Father’s Day those families would have liked to see their children too,” she said.
“We’re in this situation because the Prime Minister hasn’t got the vaccine rollout working and didn’t set up a fit for purpose quarantine system. Now that he’s back in Canberra I hope he’s spending time making sure Australians get vaccinated.
“No one wants to go through Christmas as they just did Father’s Day.”
Mr Morrison is likely to travel back to Sydney early this week.
Into the city of festering disease. I wonder how that will go.
Booster shots are in the nation’s future ACT Chief Minister Andrew Barr says a booster vaccine program will rollout through 2022, and the vaccines for that program have already been acquired.
He said those who have had the AstraZeneca vaccine will be offered an mRNA vaccine (like Pfizer or Moderna) as a booster:
“The exact details I don’t know today, but people will be advised, and there has been some discussion among health authorities in relation to those who have had the Astra Zeneca vaccine being able to have an mRNA booster, but that decision has not yet been informed by advisory groups such a ATAGI, and they will inform the nation in time,” he said.
It’s nice to see they use error bars on one part of a graph, but not another part of the same graph, where the numbers are predicted.
consider how much of a (messier and larger) dog’s breakfast it would have been if the other States had not held their borders, maintained elimination while (some of, good as), a total fucken mess it would be
stopping that bidirectional traffic across, and more, has helped a lot
later will be the big thankyou, lot of pointing with a chorus of you should open up, the superspreader will be there waiting, to help cough
Booster shots are in the nation’s future ACT Chief Minister Andrew Barr says a booster vaccine program will rollout through 2022, and the vaccines for that program have already been acquired.
He said those who have had the AstraZeneca vaccine will be offered an mRNA vaccine (like Pfizer or Moderna) as a booster:
“The exact details I don’t know today, but people will be advised, and there has been some discussion among health authorities in relation to those who have had the Astra Zeneca vaccine being able to have an mRNA booster, but that decision has not yet been informed by advisory groups such a ATAGI, and they will inform the nation in time,” he said.
ellipsis ellipsis ellipsis
Sorry we’re not up to date on chat progress yet but we’re still trying to wrap our head around this one.
Can someone with intelligence please explain it to us like we’re SCIENCE¿
That Vaccine™ is as good as the other one, right¿
That Vaccine™ makes immunity that lasts longer than the other one, right¿
We have a vast and over supply of That Vaccine™, right¿
So why is the first thing we’re hearing about any of this, that if you had That Vaccine™, then you’re going to be good to go for a booster shot with The Other Vaccine™¿
Booster shots are in the nation’s future ACT Chief Minister Andrew Barr says a booster vaccine program will rollout through 2022, and the vaccines for that program have already been acquired.
He said those who have had the AstraZeneca vaccine will be offered an mRNA vaccine (like Pfizer or Moderna) as a booster:
“The exact details I don’t know today, but people will be advised, and there has been some discussion among health authorities in relation to those who have had the Astra Zeneca vaccine being able to have an mRNA booster, but that decision has not yet been informed by advisory groups such a ATAGI, and they will inform the nation in time,” he said.
ellipsis ellipsis ellipsis
Sorry we’re not up to date on chat progress yet but we’re still trying to wrap our head around this one.
Can someone with intelligence please explain it to us like we’re SCIENCE¿
That Vaccine™ is as good as the other one, right¿
That Vaccine™ makes immunity that lasts longer than the other one, right¿
We have a vast and over supply of That Vaccine™, right¿
So why is the first thing we’re hearing about any of this, that if you had That Vaccine™, then you’re going to be good to go for a booster shot with The Other Vaccine™¿
Who’s lying¿
The have been a few studies where the results indicate that having a different vaccine to your first one may provide greater protection.
The loss of both of them in some unfortunate accident would be little mourned.
I wonder if China hate Clive enough to organise a hit…..
don’t they only organise overseas beatings / bashings, it’s the Soviets that spray spoil their friends with a nice bottle of perfume or a hot cup of tea
The loss of both of them in some unfortunate accident would be little mourned.
I wonder if China hate Clive enough to organise a hit…..
don’t they only organise overseas beatings / bashings, it’s the Soviets that spray spoil their friends with a nice bottle of perfume or a hot cup of tea
NFI. I don’t move in such exulted circles as government intelligence assimilation squads.
Comparative Number Of Deaths, 2020, According To Anyone Who Is Not A COVID-19 Alarmist
COVID-19
—
Also maybe like shark attack victims the news media could do a fact-or-pseudofactual and a sob story for each of the lives lost to COVID-19, and then we could talk party like there’s no airborne transmission.
70%-80% is OK with business and some governments because they consider that it will produce a rate of deaths that’s regrettable, but unlikely to be high enough to cause electoral backlash.
It’s the proportion of the population they’re willing to sacrifice for their aims.
70%-80% is OK with business and some governments because they consider that it will produce a rate of deaths that’s regrettable, but unlikely to be high enough to cause electoral backlash.
It’s the proportion of the population they’re willing to sacrifice for their aims.
I reckon it is going to be down to how well each state health system can cope. Once hospital get full, ICU beds are full, other surgeries cancelled, and patients being turned away – it is going to look back and make that state government look incompetent. This will be the key optic.
70%-80% is OK with business and some governments because they consider that it will produce a rate of deaths that’s regrettable, but unlikely to be high enough to cause electoral backlash.
It’s the proportion of the population they’re willing to sacrifice for their aims.
I reckon it is going to be down to how well each state health system can cope. Once hospital get full, ICU beds are full, other surgeries cancelled, and patients being turned away – it is going to look back and make that state government look incompetent. This will be the key optic.
70%-80% is OK with business and some governments because they consider that it will produce a rate of deaths that’s regrettable, but unlikely to be high enough to cause electoral backlash.
It’s the proportion of the population they’re willing to sacrifice for their aims.
70%-80% is OK with business and some governments because they consider that it will produce a rate of deaths that’s regrettable, but unlikely to be high enough to cause electoral backlash.
It’s the proportion of the population they’re willing to sacrifice for their aims.
I reckon it is going to be down to how well each state health system can cope. Once hospital get full, ICU beds are full, other surgeries cancelled, and patients being turned away – it is going to look back and make that state government look incompetent. This will be the key optic.
bad
fair
shrug probably everyone will just get used to a lower standard of living / health / care / Economy Must Grow and once you’re used to it, it’ll be back to vote for the clowns all over again shrug
shrug probably everyone will just get used to a lower standard of living / health / care / Economy Must Grow and once you’re used to it, it’ll be back to vote for the clowns all over again shrug
It’s one of the tenets of politics that the electorate will get used to anything eventually. Their short attention span and ephemeral memories soon forget that things weren’t always ‘like this’ and they just adapt to it.
The trick is to hang on in power until they forgive you for it by their forgetfulness and ignorance.
shrug probably everyone will just get used to a lower standard of living / health / care / Economy Must Grow and once you’re used to it, it’ll be back to vote for the clowns all over again shrug
It’s one of the tenets of politics that the electorate will get used to anything eventually. Their short attention span and ephemeral memories soon forget that things weren’t always ‘like this’ and they just adapt to it.
The trick is to hang on in power until they forgive you for it by their forgetfulness and ignorance.
shrug probably everyone will just get used to a lower standard of living / health / care / Economy Must Grow and once you’re used to it, it’ll be back to vote for the clowns all over again shrug
It’s one of the tenets of politics that the electorate will get used to anything eventually. Their short attention span and ephemeral memories soon forget that things weren’t always ‘like this’ and they just adapt to it.
The trick is to hang on in power until they forgive you for it by their forgetfulness and ignorance.
One day there will be no TV.
If it proves to be more of a political liability than a political tool, it may become a target.
Right now, the government has no love for the ABC, which it sees as its enemy, and not as a body which has any right to question theacts or motives of the government.
So, the government does its best to strangle the ABC via budget measures and appointments to its oversight.
It’s one of the tenets of politics that the electorate will get used to anything eventually. Their short attention span and ephemeral memories soon forget that things weren’t always ‘like this’ and they just adapt to it.
The trick is to hang on in power until they forgive you for it by their forgetfulness and ignorance.
One day there will be no TV.
If it proves to be more of a political liability than a political tool, it may become a target.
Right now, the government has no love for the ABC, which it sees as its enemy, and not as a body which has any right to question theacts or motives of the government.
So, the government does its best to strangle the ABC via budget measures and appointments to its oversight.
seems to work, they get more favourable articles from ABC these days sigh
Although SARS-CoV-2 primarily targets the respiratory system, patients with and survivors of COVID-19 can suffer neurological symptoms1,2,3. However, an unbiased understanding of the cellular and molecular processes that are affected in the brains of patients with COVID-19 is missing. Here we profile 65,309 single-nucleus transcriptomes from 30 frontal cortex and choroid plexus samples across 14 control individuals (including 1 patient with terminal influenza) and 8 patients with COVID-19. Although our systematic analysis yields no molecular traces of SARS-CoV-2 in the brain, we observe broad cellular perturbations indicating that barrier cells of the choroid plexus sense and relay peripheral inflammation into the brain and show that peripheral T cells infiltrate the parenchyma. We discover microglia and astrocyte subpopulations associated with COVID-19 that share features with pathological cell states that have previously been reported in human neurodegenerative disease4,5,6. Synaptic signalling of upper-layer excitatory neurons—which are evolutionarily expanded in humans7 and linked to cognitive function8—is preferentially affected in COVID-19. Across cell types, perturbations associated with COVID-19 overlap with those found in chronic brain disorders and reside in genetic variants associated with cognition, schizophrenia and depression. Our findings and public dataset provide a molecular framework to understand current observations of COVID-19-related neurological disease, and any such disease that may emerge at a later date.
Remember all those jokers banging on about preexisting T-cell immunity (yeah right) that we could all rely on (really), well, fair play, please tell us what they’re doing inside the brain.
Here’s a hint:
mmm… lookin’ good there¡
Wait, article says there’s no trace of SARS-CoV-2 in the brain, so it must be the other T cells (yes yes we know there are others, we’ve read books), and that must be all right then.
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
—
How Very Convenient
Labor should be putting that away for an advertising blitz come election time. Could even be a cheap one as you wouldn’t run it in Australia’s most populated state :)
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
—
How Very Convenient
I wouldn’t mind seeing the figures of vax in Liberal held seats versus Labor held.
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
—
How Very Convenient
I wouldn’t mind seeing the figures of vax in Liberal held seats versus Labor held.
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
—
How Very Convenient
I wouldn’t mind seeing the figures of vax in Liberal held seats versus Labor held.
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
—
How Very Convenient
I wouldn’t mind seeing the figures of vax in Liberal held seats versus Labor held.
It doesn’t help me much. I don’t remeber how the seats sat. 79% in Kuringai where I grew up. That’s the seat of Bradfield and the only time it swung to the left was when Jago forgot to enrol.
70%-80% is OK with business and some governments because they consider that it will produce a rate of deaths that’s regrettable, but unlikely to be high enough to cause electoral backlash.
It’s the proportion of the population they’re willing to sacrifice for their aims.
I reckon it is going to be down to how well each state health system can cope. Once hospital get full, ICU beds are full, other surgeries cancelled, and patients being turned away – it is going to look back and make that state government look incompetent. This will be the key optic.
bad
it’s an extremely dangerous biological hazard, mostly because of the extreme contagiousness, and related large part of that is its already demonstrated mutation potential
the answer to that for some is to release it, and in play right now is powerful propaganda to help release it
there isn’t any evidence to support it being legal to release it, not that i’ve seen
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
—
How Very Convenient
Labor should be putting that away for an advertising blitz come election time. Could even be a cheap one as you wouldn’t run it in Australia’s most populated state :)
https://www.youtube.com/watch?v=-YmOnJim5wU
Spanish flu vs COVID-19: An Australian perspective of a pandemic | Australian Story
finish watching^, and reading below tomorrow
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
—
How Very Convenient
Not good.
Labor states lose…
So it’s not just an inkling ..the science (stats) back it up.
Data shows NSW received 45 per cent of the Pfizer doses allocated to primary caregivers, mostly GPs, in August
Victoria, Queensland and Western Australia received less than their share of the population
Operation COVID Shield says extra doses will be provided to other states, starting with Victoria, on September 13
An analysis of publicly available data raises more questions about the way COVID-19 vaccines have been distributed in Australia since the rollout started to ramp up in the middle of the year. But the extent to which vaccine deliveries have been concentrated on NSW — at the cost of other states — may come as a surprise.
Some of that was thanks to extra vaccines, such as those in the delivery from Poland, which mostly went to NSW. But that is not the whole story and these figures illustrate the extent to which the NSW doses have come at the expense of other states.
Consider Victoria, Queensland and Western Australia, which have all seen their allocation fall well below their share of the national population. It is in the federal government-run distribution of Pfizer vaccines through the GP network — and now other primary care providers such as pharmacies — where there have been huge shifts in supply in favour of NSW.
Victoria may have missed out on up to 343,000 Pfizer jabs between June and September, Queensland 100,000 jabs and Western Australia 114,000 jabs. But more troubling is the apparent extra weighting of future Pfizer shot allocations to NSW for the remainder of the year.
The two states most adversely affected by the shift in Pfizer shots to NSW are Victoria and Queensland. 7.30 understands Queensland Health raised its concerns about the allocations with the federal government in mid-August.
—
How Very Convenient
meanwhile, yesterday Janet Young was saying that Pfizer vax was going unused in Qld because people were not taking up appts. Make of that what you will..
additionally was reading lastnight about other viruses that have some liking of endothelial cells, cause trouble that way, of which covid may be top of the list, and other stuff regard such cells in the brain blood barrier, possibly relevant to the cognitive effects of infection, or post-infection sequelae
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7943456/
Endothelial Cells in Emerging Viral Infections
additionally was reading lastnight about other viruses that have some liking of endothelial cells, cause trouble that way, of which covid may be top of the list, and other stuff regard such cells in the brain blood barrier, possibly relevant to the cognitive effects of infection, or post-infection sequelae
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7943456/
Endothelial Cells in Emerging Viral Infections
https://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrier
“The blood–brain barrier (BBB) is a highly selective semipermeable border of endothelial cells that prevents solutes in the circulating blood from non-selectively crossing into the extracellular fluid of the central nervous system where neurons reside. The blood–brain barrier is formed by endothelial cells of the capillary wall, astrocyte end-feet ensheathing the capillary, and pericytes embedded in the capillary basement membrane. This system allows the passage of some molecules by passive diffusion, as well as the selective and active transport of various nutrients, ions, organic anions, and macromolecules such as glucose, water and amino acids that are crucial to neural function.
The blood–brain barrier restricts the passage of pathogens, the diffusion of solutes in the blood, and large or hydrophilic molecules into the cerebrospinal fluid, while allowing the diffusion of hydrophobic molecules (O2, CO2, hormones) and small non-polar molecules. Cells of the barrier actively transport metabolic products such as glucose across the barrier using specific transport proteins. The barrier also restricts the passage of peripheral immune factors, like signaling molecules, antibodies, and immune cells, into the CNS, thus insulating the brain from damage due to peripheral immune events..”
additionally was reading lastnight about other viruses that have some liking of endothelial cells, cause trouble that way, of which covid may be top of the list, and other stuff regard such cells in the brain blood barrier, possibly relevant to the cognitive effects of infection, or post-infection sequelae
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7943456/
Endothelial Cells in Emerging Viral Infections
https://en.wikipedia.org/wiki/Blood%E2%80%93brain_barrier
“The blood–brain barrier (BBB) is a highly selective semipermeable border of endothelial cells that prevents solutes in the circulating blood from non-selectively crossing into the extracellular fluid of the central nervous system where neurons reside. The blood–brain barrier is formed by endothelial cells of the capillary wall, astrocyte end-feet ensheathing the capillary, and pericytes embedded in the capillary basement membrane. This system allows the passage of some molecules by passive diffusion, as well as the selective and active transport of various nutrients, ions, organic anions, and macromolecules such as glucose, water and amino acids that are crucial to neural function.
The blood–brain barrier restricts the passage of pathogens, the diffusion of solutes in the blood, and large or hydrophilic molecules into the cerebrospinal fluid, while allowing the diffusion of hydrophobic molecules (O2, CO2, hormones) and small non-polar molecules. Cells of the barrier actively transport metabolic products such as glucose across the barrier using specific transport proteins. The barrier also restricts the passage of peripheral immune factors, like signaling molecules, antibodies, and immune cells, into the CNS, thus insulating the brain from damage due to peripheral immune events..”
remember reading this article way back, or one very similar, in NS mag, talked about the BBB becoming more porous caused by stress, of course there are different sorts of stress
Just asked the doc if he had a preference for covid vaxxes. He was OK with any of them.
I also asked if there was a risk of the vax upsetting my unprecedented success with the chemo. He says it’s highly unlikely.
I’m really pleased about that as I was told by the nurse that I’m the oncology department’s poster boy for azacitadine treatment.
Just asked the doc if he had a preference for covid vaxxes. He was OK with any of them.
I also asked if there was a risk of the vax upsetting my unprecedented success with the chemo. He says it’s highly unlikely.
I’m really pleased about that as I was told by the nurse that I’m the oncology department’s poster boy for azacitadine treatment.
Just asked the doc if he had a preference for covid vaxxes. He was OK with any of them.
I also asked if there was a risk of the vax upsetting my unprecedented success with the chemo. He says it’s highly unlikely.
I’m really pleased about that as I was told by the nurse that I’m the oncology department’s poster boy for azacitadine treatment.
That shoots Margaret’s lie about her ‘doctors’ recommending against a vax. She has been in remission for a few years now…
Just asked the doc if he had a preference for covid vaxxes. He was OK with any of them.
I also asked if there was a risk of the vax upsetting my unprecedented success with the chemo. He says it’s highly unlikely.
I’m really pleased about that as I was told by the nurse that I’m the oncology department’s poster boy for azacitadine treatment.
Just asked the doc if he had a preference for covid vaxxes. He was OK with any of them.
I also asked if there was a risk of the vax upsetting my unprecedented success with the chemo. He says it’s highly unlikely.
I’m really pleased about that as I was told by the nurse that I’m the oncology department’s poster boy for azacitadine treatment.
That shoots Margaret’s lie about her ‘doctors’ recommending against a vax. She has been in remission for a few years now…
Goodonya Tamb.
The doc took a couple of months to decide. He’s very conservative.
I wonder whether the Bin-chicken will listen; all of yesterday’s deaths had “underlying conditions”. I doubt that listening will happen.
possibly the more serious underlying condition is State hate, the project of the borderblasters, given an extremely contagious pathogen they’d use it to that end, the globalist fantasy of a borderless world, any obstacle is parochial or worse, and would you pick it, contempt for borders in a premier, would you be inclined to look there
just thoughts above is all, unconcluded, possibly wrong
Government is planning October ‘firebreak’ restrictions if hospital admissions stay high
The Government has drawn up plans for an October “firebreak” Covid lockdown should hospitalisations continue at their current level and threaten to overload the NHS, a senior Government scientist has told i.
The member of the Government’s Scientific Advisory Group for Emergencies (Sage) said the UK is about to enter “an extended peak” of infections and hospitalisations, which are in danger of pushing the NHS beyond breaking point and could force the Government to re-introduce restrictions over the school half term period at the end of next month.
A full lockdown is unlikely and would be a last resort, but there are a range of measures the government could introduce.
Gutless getting everyone used to the idea that no test, no COVID-19, no dying, just Living With COVID-19® except since there are no tests to be positive, it’s Just As Good As Living Without COVID-19 isn’t it¡